-
Combunox Tablets (Forest)
DESCRIPTION
Each combination Combunox™ tablet contains:
Oxycodone HCl, USP 5 mg
Ibuprofen, USP 400 mg
Combunox is supplied in a fixed combination tablet form for oral administration and combines the opioid analgesic agent, oxycodone HCl, with the nonsteroidal anti-inflammatory (NSAID) agent, ibuprofen.
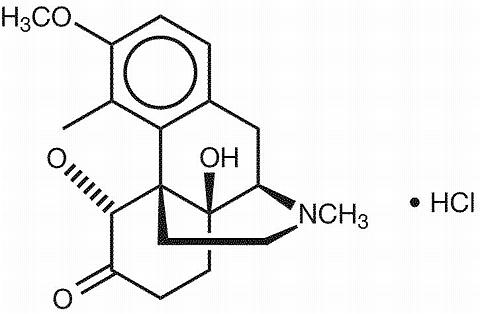
Oxycodone HCl is a centrally acting semisynthetic opioid analgesic. Its chemical name is 4,5(alpha)-Epoxy-14-hydroxy-3-methoxy-methylmorphinan-6-one hydrochloride. Its chemical formula is C 18 H 21 NO 4 HCl and molecular weight is 351.83. Its structural formula is:
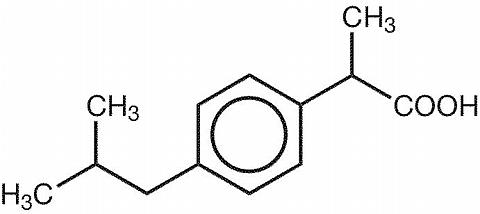
Ibuprofen is a nonsteroidal anti-inflammatory drug with analgesic and antipyretic properties. Its chemical name is (±)-2-(p-isobutylphenyl) propionic acid. Its chemical formula is C 13 H 18 O 2 and molecular weight is 206.29. Its structural formula is:
Inactive ingredients in Combunox tablets include: sodium starch glycolate, microcrystalline cellulose, colloidal silicon dioxide, stearic acid, calcium stearate, carboxymethylcellulose, povidone, Opadry® II White, Y-22 7719 coloring agent. Opadry® II White, Y-22 7719 coloring agent consists of titanium dioxide, polydextrose, hypromellose, triacetin and polyethylene glycol 8000.
CLINICAL PHARMACOLOGY
Oxycodone HCl component:
Oxycodone HCl is a semisynthetic opioid analgesic with multiple actions which involve the central nervous system and smooth muscle. The mechanism of action of oxycodone is not known but is thought to be related to its binding to opiate receptors in the central nervous system. In addition to analgesia, opioids may produce sedation and respiratory depression.
Ibuprofen component:
Ibuprofen is a nonsteroidal anti-inflammatory agent that possesses analgesic and antipyretic activities. Its mode of action, similar to other NSAIDs, is not completely understood, but is thought to be related to its inhibition of cyclooxygenase activity and prostaglandin synthesis. Ibuprofen is a peripherally acting analgesic. Ibuprofen does not have any known effects on opiate receptors.
Pharmacokinetics:
Absorption:
Oxycodone is rapidly absorbed after single dose administration of Combunox. Maximum concentrations (C max ) of oxycodone, ranging from 9.8 ng/mL to 11.7 ng/mL, are obtained within 1.3 hr to 2.1 hr after administration of Combunox. Repeated administration of Combunox every 6 hours results in approximately 50-65% increase in C max . In the presence of food, the bioavailability of oxycodone is slightly (25%) increased.
Ibuprofen is rapidly absorbed after oral administration of Combunox. C max values range from 18.5 mcg/mL to 34.3 mcg/mL and are reached 1.6 hr to 3.1 hr after oral administration of Combunox. Repeated administration of Combunox every 6 hours does not result in any accumulation of ibuprofen. The bioavailability of ibuprofen is not altered in the presence of food.
Distribution:
Oxycodone binding to protein in serum is approximately 45%.
Ibuprofen is extensively bound to plasma proteins (99%).
Metabolism:
Oxycodone is metabolized in the liver by means of N-demethylation and O-demethylation, 6-ketoreduction and glucuronidation. The major circulating metabolite is noroxycodone, which possesses weak analgesic activity.
Oxymorphone, the end product of O-demethylation, has analgesic activity but is present in the plasma at low concentrations. Metabolism of oxycodone to oxymorphone occurs via CYP2D6.
Ibuprofen is present as a racemate and following absorption, it undergoes interconversion in the plasma from the R-isomer to the S-isomer.
Both the R- and S-isomers are metabolized to two primary metabolites: (+)-2-4'-(2-hydroxy-2-methyl-propyl) phenyl propionic acid and (+)-2-4'-(2-carboxypropyl) phenyl propionic acid, both of which circulate in the plasma at low levels relative to the parent.
Elimination:
Oxycodone is eliminated from the systemic circulation with half life (T 1/2 ) values ranging from 3.1 hr to 3.7 hr after single dose administration of Combunox. Urinary excretion of unchanged oxycodone amounts to approximately 4% of the administered oxycodone dose.
Ibuprofen is eliminated from the systemic circulation with half life (T 1/2 ) values ranging from 1.8 hr to 2.6 hr after single dose administration of Combunox. Urinary excretion of unchanged ibuprofen is minimal (less than 0.2% of administered ibuprofen dose).
Special Populations:
Gender: There are no gender effects on the pharmacokinetics of oxycodone or ibuprofen after administration of Combunox.
Age: The effects of age on the pharmacokinetics of oxycodone and ibuprofen after administration of Combunox have not been evaluated.
When either drug was administered alone, the pharmacokinetics of oxycodone and ibuprofen were similar in elderly subjects, compared to young healthy subjects.
Pediatrics: The pharmacokinetics of oxycodone and ibuprofen after administration of Combunox have not been evaluated in a pediatric population.
Renal Impairment: The effects of renal impairment on the pharmacokinetics of oxycodone and ibuprofen after administration of Combunox have not been evaluated.
Hepatic Impairment: The effects of hepatic impairment on the pharmacokinetics of oxycodone and ibuprofen after administration of Combunox have not been evaluated. (See PRECAUTIONS ; Hepatic Effects )
CLINICAL STUDIES
Combunox was investigated in three clinical studies. Two studies involving a total of 949 patients following dental surgery (removal of ipsilateral molars) and a third study of 456 patients following abdominal/pelvic surgery were conducted. In the three studies patients were administered a single dose of the Combunox, ibuprofen alone, oxycodone HCl alone or placebo for acute, moderate to severe pain.
In these single dose studies, Combunox produced greater efficacy than placebo and each of Combunox's individual components as measured by the magnitude of pain relief and the reduction in pain intensity through six hours. No multiple dose efficacy studies have been performed with Combunox.
INDICATIONS AND USAGE
Combunox tablet is indicated for the short term (no more than 7 days) management of acute, moderate to severe pain.
CONTRAINDICATIONS
Combunox should not be administered to patients who have previously exhibited hypersensitivity to oxycodone HCl, ibuprofen, or any of Combunox's components, or in any situation where opioids are contraindicated. This includes patients with significant respiratory depression (in unmonitored settings or the absence of resuscitative equipment) and patients with acute or severe bronchial asthma or hypercarbia. Combunox is contraindicated in any patient who has or is suspected of having paralytic ileus. Combunox should not be given to patients who have experienced asthma, urticaria, or allergic-type reactions after taking aspirin or other NSAIDs. Severe anaphylactoid reactions to NSAIDs, some of which were fatal, have been reported in such patients (see WARNINGS - Anaphylactoid Reactions , and PRECAUTIONS - Pre-existing Asthma ). Patients known to be hypersensitive to other opioids may exhibit cross-sensitivity to oxycodone.
WARNINGS
Misuse Abuse and Diversion of Opioids
Combunox contains oxycodone, which is an opioid agonist, and a Schedule II controlled substance. Opioid agonists have the potential for being abused and are sought by abusers and people with addiction disorders, and are subject to diversion.
Combunox can be abused in a manner similar to other opioid agonists, legal or illicit. This should be considered when prescribing or dispensing Combunox in situations where the physician or pharmacist is concerned about an increased risk of misuse, abuse or diversion (see DRUG ABUSE AND DEPENDENCE ).
Respiratory Depression
Oxycodone may produce dose-related respiratory depression by acting directly on the brain stem respiratory centers. Oxycodone HCl also affects the center that controls respiratory rhythm, and may produce irregular and periodic breathing. Respiratory depression occurs most frequently in elderly or debilitated patients, usually following large initial doses in non-tolerant patients, or when opioids are given in conjunction with other agents that depress respiration. Combunox should be used with extreme caution in patients with significant chronic obstructive pulmonary disease or cor pulmonale, and in patients having substantially decreased respiratory reserve, hypoxia, hypercapnia, or pre-existing respiratory depression. In such patients, even usual therapeutic doses of Combunox may decrease respiratory drive to the point of apnea.
Hypotensive Effect
Combunox, like all opioid analgesics, may cause severe hypotension in an individual whose ability to maintain blood pressure has been compromised by a depleted blood volume, or after concurrent administration with drugs such as phenothiazines or other agents which compromise vasomotor tone. Combunox may produce orthostatic hypotension in ambulatory patients. Combunox, like all opioid analgesics, should be administered with caution to patients in circulatory shock, since vasodilatation produced by the drug may further reduce cardiac output and blood pressure.
Head Injury and Increased Intracranial Pressure
The respiratory depressant effects of opioids and their capacity to elevate cerebrospinal fluid pressure may be markedly exaggerated in the presence of head injury, intracranial lesions or a pre-existing increase in intracranial pressure. Furthermore, opioids produce adverse reactions that may obscure the clinical course of patients with head injuries.
Acute Abdominal Conditions
The administration of opioids may obscure the diagnosis or clinical course of patients with acute abdominal conditions.
Gastrointestinal (GI) Effects
Serious gastrointestinal toxicity, such as inflammation, bleeding, ulceration, and perforation of the stomach, small intestine or large intestine, can occur at any time, with or without warning symptoms, in patients treated with nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen. Minor upper GI problems, such as dyspepsia, are common and may also occur at any time during NSAID therapy. Therefore, physicians and patients should remain alert for ulceration and bleeding even in the absence of previous GI tract symptoms. Even short term therapy is not without risk.
NSAIDs should be prescribed with extreme caution in those with a prior history of ulcer disease or gastrointestinal bleeding. Most spontaneous reports of fatal GI events are in elderly or debilitated patients and, therefore, special care should be taken in treating this population. To minimize the potential risk for an adverse GI event the treatment period should be of the shortest possible duration. For high risk patients, alternate therapies that do not involve NSAIDs should be considered.
In addition to a past history of ulcer disease, pharmacoepidemiological studies have identified several other co-therapies or co-morbid conditions that may increase the risk for GI bleeding such as: treatment with oral corticosteroids, treatment with anticoagulants, longer duration of NSAID therapy, smoking, and alcoholism.
Anaphylactoid Reactions
Anaphylactoid reactions may occur in patients without known prior exposure to Combunox. Combunox should not be given to patients with the aspirin triad or a history of angioedema. The triad typically occurs in asthmatic patients who experience rhinitis with or without nasal polyps, or who exhibit severe, potentially fatal bronchospasm after taking aspirin or other NSAIDs. Fatal reactions to NSAIDs have been reported in such patients (see CONTRAINDICATIONS and PRECAUTIONS - Pre-existing Asthma ). Emergency help should be sought when anaphylactoid reaction occurs.
Advanced Renal Disease
In patients with advanced kidney disease, treatment with Combunox is not recommended. However, if Combunox therapy must be initiated, due to the NSAID component, close monitoring of the patient's kidney function is advisable (see PRECAUTIONS - Renal Effects ). If NSAID therapy, however, must be initiated, close monitoring of the patient's kidney function is advisable (see PRECAUTIONS - Renal Effects ).
Pregnancy
As with other NSAID-containing products, Combunox should be avoided in late pregnancy because it may cause premature closure of the ductus arteriosus.
Interactions with Alcohol and Drugs of Abuse
Oxycodone may be expected to have additive effects when used in conjunction with alcohol, other opioids, or illicit drugs that cause central nervous system depression.
PRECAUTIONS
General
Special Risk Patients
As with any opioid analgesic agent, Combunox tablets should be used with caution in elderly or debilitated patients, and those with severe impairment of hepatic, pulmonary or renal function, hypothyroidism, Addison's disease, acute alcoholism, convulsive disorders, CNS depression or coma, delirium tremens, kyphoscoliosis associated with respiratory depression, toxic psychosis, prostatic hypertrophy or urethral stricture. The usual precautions should be observed and the possibility of respiratory depression, postural hypotension, and altered mental states should be kept in mind.
Use in Pancreatic/Biliary Tract Disease
Combunox may cause spasm of the sphincter of Oddi and should be used with caution in patients with biliary tract disease, including acute pancreatitis. Opioids like Combunox may cause increases in the serum amylase level.
Cough Reflex
Oxycodone suppresses the cough reflex; as with other opioid containing products, caution should be exercised when Combunox is used postoperatively and in patients with pulmonary disease.
Effect on Diagnostic Signs
The antipyretic and anti-inflammatory activity of ibuprofen may reduce fever and inflammation, thus diminishing their utility as diagnostic signs in detecting complications of presumed noninfectious, noninflammatory painful conditions.
Hepatic Effects
As with other NSAIDs, ibuprofen has been reported to cause borderline elevations of one or more liver enzymes; this may occur in up to 15% of patients. These abnormalities may progress, may remain essentially unchanged, or may be transient with continued therapy. Notable (3 times the upper limit of normal) elevations of SGPT (ALT) or SGOT (AST) occurred in controlled clinical trials in less than 1% of patients. A patient with symptoms and/or signs suggesting liver dysfunction, or in whom an abnormal liver test has occurred, should be evaluated for evidence of the development of more severe hepatic reactions while on therapy with Combunox. Severe hepatic reactions, including jaundice and cases of fatal hepatitis, have been reported with ibuprofen as with other NSAIDs. Although such reactions are rare, if abnormal liver tests persist or worsen, if clinical signs and symptoms consistent with liver disease develop, or if systemic manifestations occur (e.g. eosinophilia, rash, etc.), Combunox should be discontinued.
Renal Effects
Caution should be used when initiating treatment with Combunox in patients with considerable dehydration. It is advisable to rehydrate patients first and then start therapy with Combunox. Caution is also recommended in patients with pre-existing kidney disease (see WARNINGS - Advanced Renal Disease ).
As with other NSAIDs, long-term administration of ibuprofen has resulted in renal papillary necrosis and other renal pathologic changes. Renal toxicity has also been seen in patients in which renal prostaglandins have a compensatory role in the maintenance of renal perfusion. In these patients, administration of a nonsteroidal anti-inflammatory drug may cause a dose-dependent reduction in prostaglandin formation and, secondarily, in renal blood flow, which may precipitate overt renal decompensation. Patients at greatest risk of this reaction are those with impaired renal function, heart failure, liver dysfunction, those taking diuretics and ACE inhibitors, and the elderly. Discontinuation of nonsteroidal anti-inflammatory drug therapy is usually followed by recovery to the pretreatment state.
Ibuprofen metabolites are eliminated primarily by the kidneys. The extent to which the metabolites may accumulate in patients with renal failure has not been studied. Patients with significantly impaired renal function should be more closely monitored.
Hematological Effects
Ibuprofen, like other NSAIDs, can inhibit platelet aggregation but the effect is quantitatively less and of shorter duration than that seen with aspirin. Ibuprofen has been shown to prolong bleeding time in normal subjects. Because this prolonged bleeding effect may be exaggerated in patients with underlying hemostatic defects, Combunox should be used with caution in persons with intrinsic coagulation defects and those on anticoagulant therapy. Anemia is sometimes seen in patients receiving NSAIDs, including ibuprofen. This may be due to fluid retention, GI loss, or an incompletely described effect upon erythropoiesis.
Fluid Retention and Edema
Fluid retention and edema have been reported in association with ibuprofen; therefore, the drug should be used with caution in patients with a history of cardiac decompensation, hypertension or heart failure.
Pre-existing Asthma
Patients with asthma may have aspirin-sensitive asthma. The use of aspirin in patients with aspirin-sensitive asthma has been associated with severe bronchospasm, which may be fatal. Since cross-reactivity between aspirin and other NSAIDs has been reported in such aspirin-sensitive patients, Combunox should not be administered to patients with this form of aspirin sensitivity and should be used with caution in patients with pre-existing asthma.
Aseptic Meningitis
Aseptic meningitis with fever and coma has been observed on rare occasions in patients on ibuprofen therapy. Although it is probably more likely to occur in patients with systemic lupus erythematosus and related connective tissue diseases, it has been reported in patients who do not have an underlying chronic disease. If signs or symptoms of meningitis develop in a patient on Combunox, the possibility of its being related to ibuprofen should be considered.
Information for Patients
Combunox, similar to other opioid-containing analgesics, may impair mental and/or physical abilities required for the performance of potentially hazardous tasks such as driving a car or operating machinery; patients should be cautioned accordingly.
The combination of this product with alcohol and other CNS depressants may produce an additive CNS depression and should be avoided.
Combunox can be abused in a manner similar to other opioid agonists, legal or illicit. Patients should take the drug only for as long as it is prescribed, in the amounts prescribed, and no more frequently than prescribed.
Combunox, like other drugs containing ibuprofen, is not free of side effects. The side effects of these drugs can cause discomfort and, rarely, there are more serious side effects, such as gastrointestinal bleeding, which may result in hospitalization and even fatal outcomes. Patients should be instructed to report any signs or symptoms of gastrointestinal bleeding, blurred vision or other eye problems, skin rash, weight gain, or edema.
Laboratory Tests
A decrease in hemoglobin may occur during Combunox therapy, and elevations of liver enzymes may be seen in a small percentage of patients during Combunox therapy (see PRECAUTIONS - Hematological Effects and PRECAUTIONS - Hepatic Effects ).
In patients with severe hepatic or renal disease, effects of therapy should be monitored with liver and/or renal function tests.
Drug Interactions
Oxycodone
Oxycodone is metabolized in part to oxymorphone via the cytochrome P 450 isoenzyme CYP2D6. While this pathway may be blocked by a variety of drugs (e.g., certain cardiovascular drugs and antidepressants), such blockade has not yet been shown to be of clinical significance with this agent. However, clinicians should be aware of this possible interaction.
Anticholinergics: The concurrent use of anticholinergics with oxycodone preparations may produce paralytic ileus.
CNS Depressants: Patients receiving narcotic analgesics, general anesthetics, phenothiazines, other tranquilizers, sedative-hypnotics or other CNS depressants (including alcohol) concomitantly with oxycodone may exhibit an additive CNS depression. Interactive effects resulting in respiratory depression, hypotension, profound sedation, or coma may result if these drugs are taken in combination with the usual dosage of oxycodone. When such combined therapy is contemplated, the dose of one or both agents should be reduced.
Mixed Agonist/Antagonist Opioid Analgesics: Agonist/antagonist analgesics (i.e., pentazocine, nalbuphine, butorphanol and buprenorphine) should be administered with caution to patients who have received or are receiving a course of therapy with a pure opioid agonist analgesic such as oxycodone. In this situation, mixed agonist/antagonist analgesics may reduce the analgesic effect of oxycodone and/or may precipitate withdrawal symptoms in these patients.
Monoamine Oxidase Inhibitors (MAOIs): MAOIs have been reported to intensify the effects of at least one opioid drug causing anxiety, confusion and significant depression of respiration or coma. The use of oxycodone is not recommended for patients taking MAOIs or within 14 days of stopping such treatment.
Neuromuscular Blocking Agents: Oxycodone, as well as other opioid analgesics, may enhance the neuromuscular blocking action of skeletal muscle relaxants and produce an increased degree of respiratory depression.
Ibuprofen
ACE-Inhibitors: Reports suggest that NSAIDs may diminish the antihypertensive effect of ACE-inhibitors. This interaction should be given consideration in patients taking Combunox concomitantly with ACE-inhibitors.
Aspirin: As with other products containing NSAIDs, concomitant administration of Combunox and aspirin is not generally recommended because of the potential of increased adverse effects.
Diuretics: Ibuprofen has been shown to reduce the natri-uretic effect of furosemide and thiazides in some patients. This response has been attributed to inhibition of renal prostaglandin synthesis. During concomitant therapy with Combunox the patient should be observed closely for signs of renal failure (see PRECAUTIONS - Renal Effects ), as well as diuretic efficacy.
Lithium: Ibuprofen has been shown to elevate plasma lithium concentration and reduce renal lithium clearance. This effect has been attributed to inhibition of renal prostaglandin synthesis by ibuprofen. Thus, when Combunox and lithium are administered concurrently, patients should be observed for signs of lithium toxicity.
Methotrexate: Ibuprofen, as well as other NSAIDs, has been reported to competitively inhibit methotrexate accumulation in rabbit kidney slices. This may indicate that ibuprofen could enhance the toxicity of methotrexate. Caution should be used when Combunox is administered concomitantly with methotrexate.
Warfarin: The effects of warfarin and NSAIDs on GI bleeding are synergistic, such that users of both drugs together have a greater risk of serious GI bleeding than users of either drug alone.
Carcinogenicity, Mutagenicity and Impairment of Fertility
Studies to evaluate the potential effects of the combination of oxycodone and ibuprofen on carcinogenicity, mutagenicity or impairment of fertility have not been conducted.
Pregnancy
Teratogenic Effects
Pregnancy Category C
Animal studies to assess the potential effects of the combination of oxycodone and ibuprofen on embryo-fetal development were conducted in the rat and rabbit model.
Pregnant rats were treated by oral gavage with combination doses of oxycodone:ibuprofen mg/kg/day (0.25:20, 0.5:40, 1.0:80, or 2.0:160) on days 7-16 of gestation. There was no evidence for developmental toxicity or teratogenicity at any dose, although maternal toxicity was noted at doses of 0.5:40 and above. The highest dose tested in the rat (2.00:160 mg/kg/day) is equivalent to the maximum recommended human daily dose (20:1600 mg/day) on a body surface area (mg/m 2 ) basis. This dose was associated with maternal toxicity (death, clinical signs, decreased BW).
Pregnant rabbits were treated by oral gavage with combination doses of oxycodone/ibuprofen (0.38:30, 0.75:60, 1.50:120 or 3.00:240 mg/kg/day) on gestation days 7-19. Oxycodone/ibuprofen treatment was not teratogenic under the conditions of the assay. Maternal toxicity was noted at doses of 1.5:120 (reduced body weight and food consumption) and 3:240 mg/kg/day (mortality). The NOAEL for maternal toxicity, 0.75:60 mg/kg/day, is 0.75 fold the proposed maximum daily human dose based upon the body surface area. Developmental toxicity, as evidenced by delayed ossification and reduced fetal body weights, was noted at the highest dose, which is approximately 3 times the MRHD on a mg/m 2 basis, and is likely due to maternal toxicity. The fetal no adverse effect level (NOAEL) of 1.50:120 mg/kg/day is approximately 1.5 times the MRHD on a mg/m 2 basis.
There are no adequate and well-controlled studies in pregnant women. Combunox should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Because of the ibuprofen component, Combunox should not be used during the third trimester of pregnancy because it could cause problems in the unborn child (premature closure of the ductus arteriosus and pulmonary hypertension in the fetus/neonate).
Labor and Delivery
Combunox should not be used during the third trimester of pregnancy due to the potential for ibuprofen to inhibit prostaglandin synthetase which may prolong pregnancy and inhibit labor. Oxycodone is not recommended for use in women during and immediately prior to labor and delivery because oral opioids may cause respiratory depression in the newborn.
Nursing Mothers
Ibuprofen is not transferred to breast milk in significant quantities. The American Academy of Pediatrics classified ibuprofen as compatible with breastfeeding. In studies using a 1 mcg/mL assay, ibuprofen was not detected in the milk of lactating mothers. Oxycodone is excreted in human milk. Withdrawal symptoms and/or respiratory depression have been observed in neonates whose mothers were taking narcotic analgesics during pregnancy. Although adverse effects in the nursing infant have not been documented, withdrawal can occur in breast-feeding infants when maternal administration of an opioid analgesic is discontinued.
Because of the potential for serious adverse reactions in nursing infants from the oxycodone present in Combunox, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
In the placebo-controlled, clinical studies of pain following dental surgery, 109 patients between the ages of 14 and 17 years were administered a single dose of Combunox. No apparent differences were noted in the safety of Combunox in patients below and above 17 years of age. Combunox has not been studied in patients under 14 years of age.
Geriatric Use
Of the total number of subjects in clinical studies of Combunox, 89 patients were 65 and over, while 37 patients were 75 and over. No overall differences in safety were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
However, because the elderly may be more sensitive to the renal and gastrointestinal effects of nonsteroidal anti-inflammatory agents as well as possible increased risk of respiratory depression with opioids, extra caution should be used when treating the elderly with Combunox.
ADVERSE REACTIONS
Listed below are the adverse event incidence rates from single dose analgesia trials in which a total of 2437 patients received either Combunox, ibuprofen (400 mg), oxycodone HCl (5 mg), or placebo. Adverse event information is also provided from an additional 334 patients who were exposed to Combunox in a multiple dose analgesia trial, without placebo or active component comparison arms, given up to four times daily for up to 7 days.
Adverse Events Which Occurred at a Frequency of >/= 1% and at a Higher Incidence than in the Placebo Group in Single Dose Studies 5/400 mg
(n=923)400 mg
Ibuprofen
(n=913)5 mg
Oxycodone HCl
(n = 286)Placebo
(n=315)DigestiveNausea81 (8.8%) 44 (4.8%) 46 (16.1%) 21 (6.7%) Vomiting49 (5.3%) 16 (1.8%) 30 (10.5%) 10 (3.2%) Flatulence9 (1.0%) 7 (0.8%) 3 (1.0%) 0 Nervous SystemSomnolence67 (7.3%) 38 (4.2%) 12 (4.2%) 7 (2.2%) Dizziness47 (5.1%) 21 (2.3%) 17 (5.9%) 8 (2.5%) Skin and AppendagesSweat15 (1.6%) 7 (0.8%) 4 (1.4%) 1 (0.3%)
Adverse events that were reported by at least 1% of patients taking Combunox but were observed at a greater incidence in the placebo treated patients were fever, headache and pruritus.
Adverse events that occurred in less than 1% and in at least two Combunox treated patients in Single Dose studies not listed above include the following: Body as Whole: abdominal pain, asthenia, chest pain, enlarged abdomen. Cardiovascular System: hypotension, syncope, tachycardia, vasodilation. Digestive System: constipation, dry mouth, dyspepsia, eructation, ileus. Hemic and Lymphatic System: anemia. Metabolic and Nutritional Disorders: edema. Nervous System: euphoria, insomnia, nervousness. Respiratory System: hypoxia, lung disorder, pharyngitis. Urogenital System: urinary retention.
Adverse events that occurred in the Multiple Dose study in at least 2% of patients treated with Combunox include the following: Body as Whole: asthenia (3.3%), fever (3.0%), headache (10.2%). Cardiovascular System : vasodilation (3.0%). Digestive System: constipation (4.5%), diarrhea (2.1%), dyspepsia (2.1%), nausea (25.4%), vomiting (4.5%). Nervous System: dizziness (19.2%), somnolence (17.4%).
Adverse events that occurred in less than 2% of and at least two Combunox treated patients in the Multiple Dose study not listed previously include the following: Body as Whole: back pain, chills, infection. Cardiovascular System: thrombophlebitis. Hemic and Lymphatic System: ecchymosis. Metabolic and Nutritional Disorders: hypokalemia. Musculoskeletal System: arthritis. Nervous System: abnormal thinking, anxiety, hyperkinesia, hypertonia. Skin and Appendages: rash. Special Senses: amblyopia, taste perversion. Urogenital System: urinary frequency.
DRUG ABUSE AND DEPENDENCE
Combunox contains oxycodone, which is a mu-opioid agonist with an abuse liability similar to other opioid agonists and is a Schedule II controlled substance. Combunox, and other opioids used in analgesia, can be abused and are subject to criminal diversion.
Addiction is a primary, chronic, neurobiologic disease, with genetic, psychosocial, and environmental factors influencing its development and manifestations. It is characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving. Drug addiction is a treatable disease utilizing a multidisciplinary approach, but relapse is common.
"Drug seeking" behavior is very common in addicts and drug abusers. Drug-seeking tactics include emergency calls or visits near the end of office hours, refusal to undergo appropriate examination, testing or referral, repeated "loss" of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contact information for other treating physician(s). "Doctor shopping" to obtain additional prescriptions is common among drug abusers and people suffering from untreated addiction.
Abuse and addiction are separate and distinct from physical dependence and tolerance. Physical dependence usually assumes clinically significant dimensions after several days to weeks of continuous opioid use. Tolerance, in which increasingly large doses are required in order to produce the same degree of analgesia, is manifested initially by a shorter duration of analgesic effect, and subsequently by a decrease in the intensity of analgesia. The rate of development of tolerance varies among patients. Physicians should be aware that abuse of opioids can occur in the absence of true addiction and is characterized by misuse for non-medical purposes, often in combination with other psychoactive substances. Combunox, like other opioids, may be diverted for non-medical use. Record-keeping of prescribing information, including quantity, frequency, and renewal requests is strongly advised.
Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs.
OVERDOSAGE
Following an acute overdosage, toxicity may result from oxycodone and/or ibuprofen.
Signs and Symptoms:
Acute overdosage with oxycodone may be manifested by respiratory depression, somnolence progressing to stupor or coma, skeletal muscle flaccidity, cold and clammy skin, constricted pupils, bradycardia, or hypotension. In severe cases death may occur.
The toxicity of ibuprofen overdose is dependent on the amount of drug ingested and the time elapsed since ingestion, although individual response may vary, necessitating individual evaluation of each case. Although uncommon, serious toxicity and death have been reported in the medical literature with ibuprofen overdosage. The most frequently reported symptoms of ibuprofen overdose include abdominal pain, nausea, vomiting, lethargy, and drowsiness. Other central nervous system symptoms include headache, tinnitus, CNS depression, and seizures. Cardiovascular toxicity, including hypotension, bradycardia, tachycardia, and atrial fibrillation, have also been reported.
Treatment:
In the treatment of opioid overdosage, primary attention should be given to the re-establishment of a patent airway and institution of assisted or controlled ventilation. Supportive measures (including oxygen and vasopressors) should be employed in the management of circulatory shock and pulmonary edema accompanying overdose, as indicated. Cardiac arrest or arrhythmias may require cardiac massage or defibrillation. The narcotic antagonist naloxone hydrochloride is a specific antidote against respiratory depression, which may result from overdosage or unusual sensitivity to narcotics including oxycodone. An appropriate dose of naloxone hydrochloride should be administered intravenously with simultaneous efforts at respiratory resuscitation. Since the duration of action of oxycodone may exceed that of the naloxone, the patient should be kept under continuous surveillance and repeated doses of the antagonist should be administered as needed to maintain adequate respiration. Management of hypotension, acidosis and gastrointestinal bleeding may be necessary. In cases of acute overdose, the stomach should be emptied through ipecac-induced emesis or gastric lavage. Orally administered activated charcoal may help in reducing the absorption and reabsorption of ibuprofen. Emesis is most effective if initiated within 30 minutes of ingestion. Induced emesis is not recommended in patients with impaired consciousness or overdoses greater than 400 mg/kg of the ibuprofen component in children because of the risk for convulsions and the potential for aspiration of gastric contents.
DOSAGE AND ADMINISTRATION
For the management of acute moderate to severe pain, the recommended dose of Combunox is one tablet.
Dosage should not exceed 4 tablets in a 24-hour period and should not exceed 7 days.
HOW SUPPLIED
Combunox are capsule shaped, white to off-white, film-coated tablets with "F" bisect "P" on one side and "5400" on the other side.
Bottles of 100-NDC #0456-5200-01
Storage:
Store at 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F).
A Schedule CII Narcotic
Forest Pharmaceuticals, Inc.
Subsidiary of Forest Laboratories, Inc.
St. Louis, MO 63045 USA
11/04
©2004 Forest Laboratories, Inc.
Subscribe to the "News" RSS Feed 
TOP ۞