-
Prolastin (Talecris)
FOR INTRAVENOUS USE ONLY
DESCRIPTION
Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® is a sterile, stable, lyophilized preparation of purified human Alpha 1 -Proteinase Inhibitor (alpha 1 -PI), also known as alpha 1 -antitrypsin. Prolastin is intended for use in therapy of congenital alpha 1 -antitrypsin deficiency.
Prolastin is prepared from pooled human plasma of normal donors by modification and refinements of the cold ethanol method of Cohn. 1 Part of the fractionation may be performed by another licensed manufacturer. In order to reduce the potential risk of transmission of infectious agents, Prolastin has been heat-treated in solution at 60±0.5°C for not less than 10 hours. However, no procedure has been found to be totally effective in removing viral infectivity from plasma fractionation products. In vitro studies designed to evaluate the capacity of the Prolastin manufacturing process to remove/inactivate viruses have been conducted to provide additional assurance of the viral safety profile as shown in the table below.
Process StepLog 10 Virus Reduction HIV-1 * BVDV ** PRV *** Reo **/* HAV **/* **/* PPV **/** Fractionation of Effluent I to II + III3.4 3.5 3.9 2.1 1.4 1.0 PEG Precipitation4.4 3.2 3.4 3.4 3.1 3.3 Depth Filtration>/=4.7 4.1 >/=4.7 >/=4.0 >/=2.8 >/=4.3 Pasteurization>/=6.3 4.8 >/=4.8 N/A N/A N/A Accumulated Log 10 Reduction>/=18.8 15.6 >/=16.8 >/=9.5 >/=7.3 >/=8.6 *Human immunodeficiency virus, type 1 ** Bovine viral diarrhea virus (BVDV) was chosen to model hepatitis C virus *** Pseudorabies virus (PRV) was used as a surrogate for hepatitis B virus and the human herpes viruses **/* Reovirus type 3 (Reo) was chosen to model non-enveloped viruses **/* **/* Human hepatitis A virus (HAV). **/** Porcine parvovirus (PPV) was selected as a surrogate for human parvovirus B19 The specific activity of Prolastin is >/=0.35 mg functional alpha 1 -PI/mg protein and when reconstituted as directed, the concentration of alpha 1 -PI is >/=20 mg/mL. When reconstituted, Prolastin has a pH of 6.6-7.4, a sodium content of 100-210 mEq/L, a chloride content of 60-180 mEq/L, a sodium phosphate content of 0.015-0.025 M, a polyethylene glycol content of not more than (NMT) 5 ppm, and NMT 0.1% sucrose. Prolastin contains small amounts of other plasma proteins including alpha 2 -plasmin inhibitor, alpha 1 -antichymotrypsin, C 1 -esterase inhibitor, haptoglobin, antithrombin III, alpha 1 -lipoprotein, albumin, and IgA. 1
Each vial of Prolastin contains the labeled amount of functionally active alpha 1 -PI in milligrams per vial (mg/vial), as determined by capacity to neutralize porcine pancreatic elastase. 1 Prolastin contains no preservative and must be administered by the intravenous route.
CLINICAL PHARMACOLOGY
Alpha 1 -antitrypsin deficiency is a chronic, hereditary, usually fatal, autosomal recessive disorder in which a low concentration of alpha 1 -PI (alpha 1 -antitrypsin) is associated with slowly progressive, severe panacinar emphysema that most often manifests itself in the third to fourth decades of life. 2-9 [Although the terms "Alpha 1 -Proteinase Inhibitor" and "alpha 1 -antitrypsin" are used interchangeably in the scientific literature, the hereditary disorder associated with a reduction in the serum level of alpha 1 -PI is conventionally referred to as "alpha 1 -antitrypsin deficiency" while the deficient protein is referred to as "Alpha 1 -Proteinase Inhibitor" 10 ]. The emphysema is typically worse in the lower lung zones. 4,8,9 The pathogenesis of development of emphysema in alpha 1 -antitrypsin deficiency is not well understood at this time. It is believed, however, to be due to a chronic biochemical imbalance between elastase (an enzyme capable of degrading elastin tissues, released by inflammatory cells, primarily neutrophils, in the lower respiratory tract) and alpha 1 -PI (the principal inhibitor of neutrophil elastase), which is deficient in alpha 1 -antitrypsin disease. 11-15 As a result, it is believed that alveolar structures are unprotected from chronic exposure to elastase released from a chronic, low-level burden of neutrophils in the lower respiratory tract, resulting in progressive degradation of elastin tissues. 11-15 The eventual outcome is the development of emphysema. Neonatal hepatitis with cholestatic jaundice appears in approximately 10% of newborns with alpha 1 -antitrypsin deficiency. 15 In some adults, alpha 1 -antitrypsin deficiency is complicated by cirrhosis. 15
A large number of phenotypic variants of alpha 1 -antitrypsin deficiency exists. 15 The most severely affected individuals are those with the PiZZ variant, typically characterized by alpha 1 -PI serum levels <35% normal. 15 Epidemiologic studies of individuals with various phenotypes of alpha 1 antitrypsin deficiency have demonstrated that individuals with endogenous serum levels of alpha 1 -PI </=50 mg/dL (based on commercial standards) have a risk of >80% of developing emphysema over a lifetime. 3-6,8,9,16 However, individuals with endogenous alpha 1 -PI levels >80 mg/dL, in general, do not manifest an increased risk for development of emphysema above the general population background risk. 5,15 From these observations, it is believed that the "threshold" level of alpha 1 -PI in the serum required to provide adequate anti-elastase activity in the lung of individuals with alpha 1 -antitrypsin deficiency is about 80 mg/dL (based on commercial standards for immunologic assay of alpha 1 -PI). 12,15,17
In clinical studies of Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® , 23 subjects with the PiZZ variant of congenital deficiency of alpha 1 -antitrypsin deficiency and documented destructive lung disease participated in a study of acute and/or chronic replacement therapy with Prolastin. 18 The mean in vivo recovery of alpha 1 -PI was 4.2 mg (immunologic)/dL per mg (functional)/kg body weight administered. 18,19 The half-life of alpha 1 -PI in vivo was approximately 4.5 days. 18,19 Based on these observations, a program of chronic replacement therapy was developed. Nineteen of the subjects in these studies received Prolastin replacement therapy, 60 mg/kg body weight, once weekly for up to 26 weeks (average 24 weeks of therapy). With this schedule of replacement therapy, blood levels of alpha 1 -PI were maintained above 80 mg/dL (based on the commercial standards for alpha 1 -PI immunologic assay). 18-20 Within a few weeks of commencing this program, bronchoalveolar lavage studies demonstrated significantly increased levels of alpha 1 -PI and functional antineutrophil elastase capacity in the epithelial lining fluid of the lower respiratory tract of the lung, as compared to levels prior to commencing the program of chronic replacement therapy with Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® . 18-20
All 23 individuals who participated in the investigations were immunized with Hepatitis B Vaccine and received a single dose of Hepatitis B Immune Globulin (Human) on entry into the investigation. Although no other steps were taken to prevent hepatitis, neither hepatitis B nor non-A, non-B hepatitis occurred in any of the subjects. 18,19 All subjects remained seronegative for HIV antibody. None of the subjects developed any detectable antibody to alpha 1 -PI or other serum protein.
Long-term controlled clinical trials to evaluate the effect of chronic replacement therapy with Prolastin on the development of or progression of emphysema in patients with congenital alpha 1 -antitrypsin deficiency have not been performed. Estimates of the sample size required of this rare disorder and the slow, progressive nature of the clinical course have been considered impediments in the ability to conduct such a trial. 21 Studies to monitor the long-term effects will continue as part of the postapproval process.
INDICATIONS AND USAGE
Congenital Alpha 1 -Antitrypsin Deficiency
Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® is indicated for chronic replacement therapy of individuals having congenital deficiency of alpha 1 -PI (alpha 1 -antitrypsin deficiency) with clinically demonstrable panacinar emphysema. Clinical and biochemical studies have demonstrated that with such therapy, it is possible to increase plasma levels of alpha 1 -PI, and that levels of functionally active alpha 1 -PI in the lung epithelial lining fluid are increased proportionately. 18-20 As some individuals with alpha 1 -antitrypsin deficiency will not go on to develop panacinar emphysema, only those with evidence of such disease should be considered for chronic replacement therapy with Prolastin. 22 Subjects with the PiMZ or PiMS phenotypes of alpha 1 -antitrypsin deficiency should not be considered for such treatment as they appear to be at small risk for panacinar emphysema. 22 Clinical data are not available as to the long-term effects derived from chronic replacement therapy of individuals with alpha 1 -antitrypsin deficiency with Prolastin. Only adult subjects have received Prolastin to date.
Prolastin is not indicated for use in patients other than those with PiZZ, PiZ(null) or Pi(null)(null) phenotypes.
CONTRAINDICATIONS
Individuals with selective IgA deficiencies who have known antibody against IgA (anti-IgA antibody) should not receive Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® , since these patients may experience severe reactions, including anaphylaxis, to IgA which may be present.
WARNINGS
Because this product is made from human blood, it may carry a risk of transmitting infectious agents, e.g. viruses, and, theoretically, the Creutzfeldt-Jakob (CJD) agent. The risk that such products will transmit an infectious agent has been reduced by screening plasma donors for prior exposure to certain viruses, by testing for the presence of certain current virus infections, and by inactivating and/or removing certain viruses. Despite these measures, such products can still potentially transmit disease. There is also the possibility that unknown infectious agents may be present in such products. Individuals who receive infusions of blood or plasma products may develop signs and/or symptoms of some viral infections, particularly hepatitis C. ALL infections thought by a physician possibly to have been transmitted by this product should be reported by the physician or other healthcare provider to Talecris Biotherapeutics, Inc. [1-800-520-2807].
The physician should discuss the risks and benefits of this product with the patient, before prescribing or administering it to a patient.
Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® has been heat-treated in solution at 60°C for 10 hours in order to reduce the potential for transmission of infectious agents. 1 No cases of hepatitis, either hepatitis B or hepatitis C, have been recorded to date in individuals receiving Prolastin. 18 However, as all individuals received prophylaxis against hepatitis B, no conclusion can be drawn at this time regarding potential transmission of hepatitis B virus.
PRECAUTIONS
General
- Administer within 3 hours after reconstitution. Do not refrigerate after reconstitution.
- Administer only by the intravenous route.
- As with any colloid solution, there will be an increase in plasma volume following intravenous administration of Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® . 23 Caution should therefore be used in patients at risk for circulatory overload.
- Prolastin should be given alone, without mixing with other agents or diluting solutions.
-
Product administration and handling of the needles must be done with caution. Percutaneous puncture with a needle contaminated with blood can transmit infectious virus including HIV (AIDS) and hepatitis. Obtain immediate medical attention if injury occurs.
Place needles in sharps container after single use. Discard all equipment including any reconstituted Prolastin product in accordance with biohazard procedures.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies in animals to evaluate carcinogenesis, mutagenesis, or impairment of fertility have not been conducted.
Pregnancy Category C
Animal reproduction studies have not been conducted with Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® . It is also not known whether Prolastin can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. Prolastin should be given to a pregnant woman only if clearly needed.
Nursing Mothers
It is not known whether Prolastin is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Prolastin is administered to a nursing woman.
Pediatric Use
Safety and effectiveness in the pediatric population have not been established.
ADVERSE REACTIONS
Therapeutic administration of Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® , 60 mg/kg weekly, has been demonstrated to be well tolerated. In clinical studies, six reactions were observed with 517 infusions of Prolastin, or 1.16%. None of the reactions was severe. 18 The adverse reactions reported included delayed fever (maximum temperature rise was 38.9°C, resolving spontaneously over 24 hours) occurring up to 12 hours following treatment (0.77%), light-headedness (0.19%), and dizziness (0.19%). 18 Mild transient leukocytosis and dilutional anemia several hours after infusion have also been noted. 18 Since market entry, occasional reports of other flu-like symptoms, allergic-like reactions, chills, dyspnea, rash, tachycardia, and, rarely, hypotension have also been received. Rare cases of transient increase in blood pressure or hypertension and chest pain have also been reported.
DOSAGE AND ADMINISTRATION
FOR INTRAVENOUS USE ONLY
Each bottle of Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® has the functional activity, as determined by inhibition of porcine pancreatic elastase, 1 stated on the label of the bottle.
The "threshold" level of alpha 1 -PI in the serum believed to provide adequate anti-elastase activity in the lung of individuals with alpha 1 -antitrypsin deficiency is 80 mg/dL (based on commercial standards for alpha 1 -PI immunologic assay). 12,15,17 However, assays of alpha 1 -PI based on commercial standards measure antigenic activity of alpha 1 -PI, whereas the labeled potency value of alpha 1 -PI is expressed as actual functional activity, i.e., actual capacity to neutralize porcine pancreatic elastase. As functional activity may be less than antigenic activity, serum levels of alpha 1 -PI determined using commercial immunologic assays may not accurately reflect actual functional alpha 1 -PI levels. Therefore, although it may be helpful to monitor serum levels of alpha 1 -PI in individuals receiving Prolastin, using currently available commercial assays of antigenic activity, results of these assays should not be used to determine the required therapeutic dosage.
The recommended dosage of Prolastin is 60 mg/kg body weight administered once weekly. This dose is intended to increase and maintain a level of functional alpha 1 -PI in the epithelial lining of the lower respiratory tract, providing adequate anti-elastase activity in the lung of individuals with alpha 1 -antitrypsin deficiency.
Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® may be given at a rate of 0.08 mL/kg/min or greater and must be administered intravenously. The recommended dosage of 60 mg/kg takes approximately 30 minutes to infuse.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit.
Safety and effectiveness in pediatric patients has not been established.
Reconstitution
Vacuum Transfer
Note: Aseptic technique should be carefully followed. All needles and vial tops that will come into contact with the product to be administered via the intravenous route should not come in contact with any nonsterile surface. Any contaminated needles should be discarded by placing in a puncture-proof container and new equipment should be used.
- After removing all items from the box, warm the sterile water (diluent) to room temperature (25°C, 77°F)
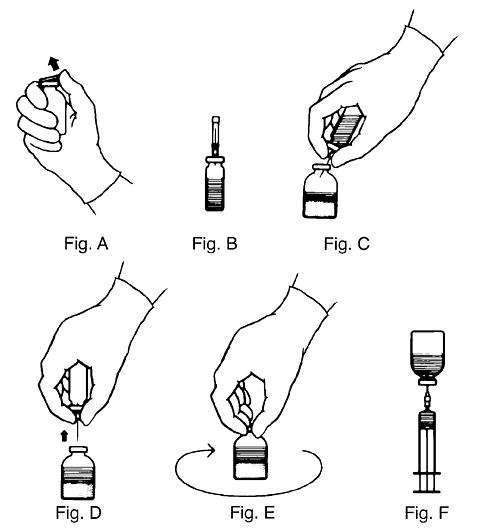
- Remove the plastic flip tops from each vial (Fig. A). Cleanse vial tops (grey stoppers) with alcohol swab and allow surface to dry. After cleaning, do not allow anything to touch the latex (rubber) stopper.
- Carefully remove the plastic sheath from the short end of the transfer needle. Insert the exposed needle into the diluent vial to the hub (Fig. B).
- Carefully grip the sheath of the other end of the transfer needle and twist to remove it.
- Invert the diluent vial and insert the attached needle into the vial of concentrate at a 45° angle (Fig. C). This will direct the stream of diluent against the wall of the concentrate vial and minimize foaming. The vacuum will draw the diluent into the concentrate vial.
- Remove the diluent bottle and transfer needle (Fig. D).
- Gently swirl the concentrate bottle until the powder is completely dissolved (Fig. E). The vial should then be visually inspected for particulate matter and discoloration prior to administration.
- Clean the top of the vial of reconstituted Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® again with alcohol swab and let surface dry.
- Attach the filter needle (from the package) to sterile syringe. Withdraw the Prolastin solution into the syringe through the filter needle (Fig. F).
- Remove the filter needle from the syringe and replace with an appropriate injection needle for administration. Discard filter needle into a puncture-proof container.
- The contents of more than one bottle of Prolastin may be drawn into the same syringe before administration. If more than one bottle of Prolastin is used, withdraw contents from bottles using aseptic technique. Place contents into an administration container (plastic minibag or glass bottle) using a syringe. * Avoid pushing an I.V. administration set spike into the product container stopper as this has been known to force the stopper into the vial, with a resulting loss of sterility.
*For a patient of average weight (about 70 kg) the volume needed will exceed the limit of one syringe.
A number of factors beyond our control could reduce the efficacy of this product or even result in an ill effect following its use. These include improper storage and handling of the product after it leaves our hands, diagnosis, dosage, method of administration, and biological differences in individual patients. Because of these factors, it is important that this product be stored properly, that the directions be followed carefully during use, and that the risk of transmitting viruses be carefully weighed before the product is prescribed.
HOW SUPPLIED
Alpha 1 -Proteinase Inhibitor (Human), Prolastin ® is supplied in the following single use vials with the total alpha 1 -PI functional activity, in milligrams, stated on the label of each vial. A suitable volume of Sterile Water for Injection, USP, is provided.
NDC Number Approximate Alpha 1 -PI
Functional ActivityDiluent 13533-601-30 500 mg 20 mL 13533-601-35 1000 mg 40 mL STORAGE
Prolastin should be stored at temperatures not to exceed 25°C (77°F). Freezing should be avoided as breakage of the diluent bottle might occur.
Rx only
REFERENCES
- Coan MH, Brockway WJ, Eguizabal H, et al: Preparation and properties of alpha 1 -proteinase inhibitor concentrate from human plasma. Vox Sang 48(6):333-42, 1985.
- Laurell CB, Eriksson S: The electrophoretic alpha 1 globulin pattern of serum in alpha 1 -antitrypsin deficiency. Scand J Clin Lab Invest 15:132-40, 1963.
- Eriksson S: Pulmonary emphysema and alpha 1 antitrypsin deficiency. Acta Med Scand 175(2):197-205, 1964.
- Eriksson S: Studies in alpha 1 -antitrypsin deficiency. Acta Med Scand Suppl 432:1-85, 1965.
- Kueppers F, Black LF: Alpha 1 -antitrypsin and its deficiency. Am Rev Respir Dis 110(2):176-94, 1974.
- Morse JO: Alpha 1 -antitrypsin deficiency. N Engl J Med 299:1045-8; 1099-105, 1978.
- Black LF, Kueppers F: Alpha 1 -antitrypsin deficiency in nonsmokers. Am Rev Respir Dis 117(3):421-8, 1978.
- Tobin MJ, Cook PJ, Hutchison DC: Alpha 1 -antitrypsin deficiency: the clinical and physiological features of pulmonary emphysema in subjects homozygous for Pi type Z. A survey by the British Thoracic Association. Br J Dis Chest 77(1):14-27, 1983.
- Larsson C: Natural history and life expectancy in severe alpha 1 -antitrypsin deficiency, Pi Z. Acta Med Scand 204(5): 345-51, 1978.
- Pannell R, Johnson D, Travis J: Isolation and properties of human plasma alpha 1 -proteinase inhibitor. Biochemistry 13(26):5439-45, 1974.
- Lieberman J: Elastase, collagenase, emphysema, and alpha 1 -antitrypsin deficiency. Chest 70(1):62-7, 1976.
- Gadek JE, Fells GA, Zimmerman RL, et al: Antielastases of the human alveolar structures: implications for the protease-antiprotease theory of emphysema. J Clin Invest 68(4):889-98, 1981.
- Beatty K, Bieth J, Travis J: Kinetics of association of serine proteinases with native and oxidized alpha-1-proteinase inhibitor and alpha-1-antichymotrypsin. J Biol Chem 255(9):3931-4, 1980.
- Janoff A, White R, Carp H, et al: Lung injury induced by leukocytic proteases. Am J Pathol 97(1):111-36, 1979.
- Gadek JE, Crystal RG: Alpha 1 -antitrypsin deficiency. In: Stanbury JB, Wyngaarden JB, Frederickson DS, et al, eds.: The Metabolic Basis of Inherited Disease. 5th ed. New York, McGraw-Hill, 1983, p.1450-67.
- Larsson C, Dirksen H, Sundstrom G, et al: Lung function studies in asymptomatic individuals with moderately (Pi SZ) and severely (Pi Z) reduced levels of alpha 1 -antitrypsin. Scand J Respir Dis 57(6):267-80, 1976.
- Gadek JE, Klein HG, Holland PV, et al: Replacement therapy of alpha 1 -antitrypsin deficiency: reversal of protease-antiprotease imbalance within the alveolar structures of PiZ subjects. J Clin Invest 68(5):1158-65, 1981.
- Data on file.
- Wewers MD, Casolaro MA, Sellers SE, et al: Replacement therapy for alpha 1 -antitrypsin deficiency associated with emphysema. N Engl J Med 316(17):1055-62,1987.
- Wewers MD, Casolaro MA, Crystal RG: Comparison of alpha-1-antitrypsin levels and antineutrophil elastase capacity of blood and lung in a patient with the alpha-1-antitrypsin phenotype null-null before and during alpha-1-antitrypsin augmentation therapy. Am Rev Respir Dis 135(3):539-43, 1987.
- Burrows B: A clinical trial of efficacy of antiproteo-lytic therapy: can it be done? Am Rev Respir Dis 127(2:2):S42-3, 1983.
- Cohen AB: Unraveling the mysteries of alpha 1 -antitrypsin deficiency. N Engl J Med 314(12):778-9, 1986.
- Finlayson JS: Albumin products. Semin Thromb Hemost 6(2):85-120, 1980.
08908802 (Rev. January 2005)
Talecris Biotherapeutics, Inc.
Research Triangle Park, NC 27709 USA
U.S. License No. 1716
Subscribe to the "News" RSS Feed 
TOP ۞