-
Rapamune Oral Solution and Tablets (Wyeth)
This product's label may have been revised after this insert was used in production. For further product information and current package insert, please visit www.wyeth.com or call our medical communications department toll-free at 1-800-934-5556.
WARNING:
Increased susceptibility to infection and the possible development of lymphoma may result from immunosuppression. Only physicians experienced in immunosuppressive therapy and management of renal transplant patients should use Rapamune ® . Patients receiving the drug should be managed in facilities equipped and staffed with adequate laboratory and supportive medical resources. The physician responsible for maintenance therapy should have complete information requisite for the follow-up of the patient.
DESCRIPTION
Rapamune ® (sirolimus) is an immunosuppressive agent. Sirolimus is a macrocyclic lactone produced by Streptomyces hygroscopicus . The chemical name of sirolimus (also known as rapamycin) is (3 S ,6 R ,7 E ,9 R ,10 R ,12 R ,14 S ,15 E ,17 E ,19 E ,21 S ,23 S ,26 R ,27 R ,34a S )-9,10,12,13,14,21,22,23,24,25,26,27,32,33,34, 34a-hexadecahydro-9,27-dihydroxy-3-[(1 R )-2-[(1 S ,3 R ,4 R )-4-hydroxy-3-methoxycyclohexyl]-1-methylethyl]-10,21-dimethoxy-6,8,12,14,20,26-hexamethyl-23,27-epoxy-3 H -pyrido[2,1-c][1,4] oxaazacyclohentriacontine-1,5,11,28,29 (4 H ,6 H ,31 H )-pentone. Its molecular formula is C 51 H 79 NO 13 and its molecular weight is 914.2. The structural formula of sirolimus is shown below.
Sirolimus is a white to off-white powder and is insoluble in water, but freely soluble in benzyl alcohol, chloroform, acetone, and acetonitrile.
Rapamune ® is available for administration as an oral solution containing 1 mg/mL sirolimus. Rapamune is also available as a white, triangular-shaped tablet containing 1-mg sirolimus, and as a yellow to beige triangular-shaped tablet containing 2-mg sirolimus.
The inactive ingredients in Rapamune ® Oral Solution are Phosal 50 PG ® (phosphatidylcholine, propylene glycol, mono- and di-glycerides, ethanol, soy fatty acids, and ascorbyl palmitate) and polysorbate 80. Rapamune Oral Solution contains 1.5% - 2.5% ethanol.
The inactive ingredients in Rapamune ® Tablets include sucrose, lactose, polyethylene glycol 8000, calcium sulfate, microcrystalline cellulose, pharmaceutical glaze, talc, titanium dioxide, magnesium stearate, povidone, poloxamer 188, polyethylene glycol 20,000, glyceryl monooleate, carnauba wax, and other ingredients. The 2 mg dosage strength also contains iron oxide yellow 10 and iron oxide brown 70.
CLINICAL PHARMACOLOGY
Mechanism of Action
Sirolimus inhibits T lymphocyte activation and proliferation that occurs in response to antigenic and cytokine (Interleukin [IL]-2, IL-4, and IL-15) stimulation by a mechanism that is distinct from that of other immunosuppressants. Sirolimus also inhibits antibody production. In cells, sirolimus binds to the immunophilin, FK Binding Pro-tein-12 (FKBP-12), to generate an immunosuppressive complex. The sirolimus:FKBP-12 complex has no effect on calcineurin activity. This complex binds to and inhibits the activation of the mammalian Target Of Rapamycin (mTOR), a key regulatory kinase. This inhibition suppresses cytokine-driven T-cell proliferation, inhibiting the progression from the G 1 to the S phase of the cell cycle.
Studies in experimental models show that sirolimus prolongs allograft (kidney, heart, skin, islet, small bowel, pancreatico-duodenal, and bone marrow) survival in mice, rats, pigs, and/or primates. Sirolimus reverses acute rejection of heart and kidney allografts in rats and prolongs the graft survival in presensitized rats. In some studies, the immunosuppressive effect of sirolimus lasts up to 6 months after discontinuation of therapy. This tolerization effect is alloantigen specific.
In rodent models of autoimmune disease, sirolimus suppresses immune-mediated events associated with systemic lupus erythematosus, collagen-induced arthritis, autoimmune type I diabetes, autoimmune myocarditis, experimental allergic encephalomyelitis, graft-versus-host disease, and autoimmune uveoretinitis.
Pharmacokinetics
Sirolimus pharmacokinetic activity has been determined following oral administration in healthy subjects, pediatric patients, hepatically-impaired patients, and renal transplant patients.
Absorption
Following administration of Rapamune ® Oral Solution, sirolimus is rapidly absorbed, with a mean time-to-peak concentration (t max ) of approximately 1 hour after a single dose in healthy subjects and approximately 2 hours after multiple oral doses in renal transplant recipients. The systemic availability of sirolimus was estimated to be approximately 14% after the administration of Rapamune Oral Solution. The mean bioavailability of sirolimus after administration of the tablet is about 27% higher relative to the oral solution. Sirolimus oral tablets are not bioequivalent to the oral solution; however, clinical equivalence has been demonstrated at the 2-mg dose level. (See CLINICAL STUDIES and DOSAGE AND ADMINISTRATION ). Sirolimus concentrations, following the administration of Rapamune Oral Solution to stable renal transplant patients, are dose proportional between 3 and 12 mg/m 2 .
Food effects: In 22 healthy volunteers receiving Rapamune Oral Solution, a high-fat meal (861.8 kcal, 54.9% kcal from fat) altered the bioavailability characteristics of sirolimus. Compared with fasting, a 34% decrease in the peak blood sirolimus concentration (C max ), a 3.5-fold increase in the time-to-peak concentration (t max ), and a 35% increase in total exposure (AUC) was observed. After administration of Rapamune Tablets and a high-fat meal in 24 healthy volunteers, C max , t max , and AUC showed increases of 65%, 32%, and 23%, respectively. To minimize variability, both Rapamune Oral Solution and Tablets should be taken consistently with or without food (See DOSAGE AND ADMINISTRATION ).
Distribution
The mean (± SD) blood-to-plasma ratio of sirolimus was 36 ± 18 in stable renal allograft recipients after administration of oral solution, indicating that sirolimus is extensively partitioned into formed blood elements. The mean volume of distribution (V ss /F) of sirolimus is 12 ± 8 L/kg. Sirolimus is extensively bound (approximately 92%) to human plasma proteins. In man, the binding of sirolimus was shown mainly to be associated with serum albumin (97%), (alpha) 1 -acid glycoprotein, and lipoproteins.
Metabolism
Sirolimus is a substrate for both cytochrome P450 IIIA4 (CYP3A4) and P-glycoprotein (P-gp). Sirolimus is extensively metabolized by the CYP3A4 isozyme in the intestinal wall and liver and undergoes counter-transport from enterocytes of the small intestine into the gut lumen by the P-gp drug efflux pump. Sirolimus is potentially recycled between enterocytes and the gut lumen to allow continued metabolism by CYP3A4. Therefore, absorption and subsequent elimination of systemically absorbed sirolimus may be influenced by drugs that affect these proteins. Inhibitors of CYP3A4 and P-gp increase sirolimus concentrations. Inducers of CYP3A4 and P-gp decrease sirolimus concentrations. (See WARNINGS and PRECAUTIONS , Drug Interactions and Other drug interactions ). Sirolimus is extensively metabolized by O-demethylation and/or hydroxylation. Seven (7) major metabolites, including hydroxy, demethyl, and hydroxydemethyl, are identifiable in whole blood. Some of these metabolites are also detectable in plasma, fecal, and urine samples. Glucuronide and sulfate conjugates are not present in any of the biologic matrices. Sirolimus is the major component in human whole blood and contributes to more than 90% of the immunosuppressive activity.
Excretion
After a single dose of [ 14 C]sirolimus oral solution in healthy volunteers, the majority (91%) of radioactivity was recovered from the feces, and only a minor amount (2.2%) was excreted in urine.
Pharmacokinetics in renal transplant patients
Rapamune Oral Solution: Pharmacokinetic parameters for sirolimus oral solution given daily in combination with cyclosporine and corticosteroids in renal transplant patients are summarized below based on data collected at months 1, 3, and 6 after transplantation (Studies 1 and 2; see CLINICAL STUDIES ). There were no significant differences in any of these parameters with respect to treatment group or month.
SIROLIMUS PHARMACOKINETIC PARAMETERS (MEAN ± SD) IN RENAL
TRANSPLANT PATIENTS (MULTIPLE DOSE ORAL SOLUTION) a , bN Dose C max,ss c
(ng/mL)t max,ss
(h)AUC [tgr ],ss c
(ng·h/mL)CL/F/WT d
(mL/h/kg)19 2 mg 12.2 ± 6.2 3.01 ± 2.40 158 ± 70 182 ± 72 23 5 mg 37.4 ± 21 1.84 ± 1.30 396 ± 193 221 ± 143 a: Sirolimus administered four hours after cyclosporine oral solution (MODIFIED) (e.g., Neoral ® Oral Solution) and/or cyclosporine capsules (MODIFIED) (e.g., Neoral ® Soft Gelatin Capsules). b: As measured by the Liquid Chromatographic/Tandem Mass Spectrometric Method (LC/MS/MS). c: These parameters were dose normalized prior to the statistical comparison. d: CL/F/WT = oral dose clearance.
Whole blood sirolimus trough concentrations (mean ± SD), as measured by immunoassay, for the 2 mg/day and 5 mg/day dose groups were 8.6 ± 4.0 ng/mL (n = 226) and 17.3 ± 7.4 ng/mL (n = 219), respectively. Whole blood trough sirolimus concentrations, as measured by LC/MS/MS, were significantly correlated (r 2 =0.96) with AUC [tgr ],ss . Upon repeated twice daily administration without an initial loading dose in a multiple-dose study, the average trough concentration of sirolimus increases approximately 2 to 3-fold over the initial 6 days of therapy at which time steady state is reached. A loading dose of 3 times the maintenance dose will provide near steady-state concentrations within 1 day in most patients. The mean ± SD terminal elimination half life (t ½ ) of sirolimus after multiple dosing in stable renal transplant patients was estimated to be about 62 ± 16 hours.
Rapamune Tablets: Pharmacokinetic parameters for sirolimus tablets administered daily in combination with cyclosporine and corticosteroids in renal transplant patients are summarized below based on data collected at months 1 and 3 after transplantation (Study 3; see CLINICAL STUDIES ).
SIROLIMUS PHARMACOKINETIC PARAMETERS (MEAN ± SD) IN RENAL
TRANSPLANT PATIENTS (MULTIPLE DOSE TABLETS) a , bn Dose
(2 mg/day)C max,ss c
(ng/mL)t max,ss
(h)AUC [tgr ],ss c
(ng·h/mL)CL/F/WT d
(mL/h/kg)17 Oral solution 14.4 ± 5.3 2.12 ± 0.84 194 ± 78 173 ± 50 13 Tablets 15.0 ± 4.9 3.46 ± 2.40 230 ± 67 139 ± 63 a: Sirolimus administered four hours after cyclosporine oral solution (MODIFIED) (e.g., Neoral ® Oral Solution) and/or cyclosporine capsules (MODIFIED) (e.g., Neoral ® Soft Gelatin Capsules). b: As measured by the Liquid Chromatographic/Tandem Mass Spectrometric Method (LC/MS/MS). c: These parameters were dose normalized prior to the statistical comparison. d: CL/F/WT = oral dose clearance.
Whole blood sirolimus trough concentrations (mean ± SD), as measured by immunoassay, for 2 mg of oral solution and 2 mg of tablets over 6 months, were 8.9 ± 4.4 ng/mL(n = 172) and 9.5 ± 3.9 ng/mL (n = 179), respectively. Whole blood trough sirolimus concentrations, as measured by LC/MS/MS, were significantly correlated (r 2 = 0.85) with AUC [tgr ],ss . Mean whole blood sirolimus trough concentrations in patients receiving either Rapamune Oral Solution or Rapamune Tablets with a loading dose of three times the maintenance dose achieved steady-state concentrations within 24 hours after the start of dose administration.
Average Rapamune doses and sirolimus whole blood trough concentrations for tablets administered daily in combination with cyclosporine and following cyclosporine withdrawal, in combination with corticosteroids in renal transplant patients (Study 4; see CLINICAL STUDIES ) are summarized in the table below.
AVERAGE RAPAMUNE DOSES AND SIROLIMUS TROUGH CONCENTRATIONS (MEAN ± SD) IN RENAL TRANSPLANT PATIENTS AFTER MULTIPLE DOSE TABLET ADMINISTRATION Rapamune with
Cyclosporine Therapy aRapamune Following
Cyclosporine Withdrawal aRapamune Dose (mg/day)Months 4 to 122.1 ± 0.7 8.2 ± 4.2 Months 12 to 242.0 ± 0.8 6.4 ± 3.0 Sirolimus C min , (ng/mL) bMonths 4 to 1210.7 ± 3.8 23.3 ± 5.0 Months 12 to 2411.2 ± 4.1 22.5 ± 4.8 a: 215 patients were randomized to each group.b: Expressed by immunoassay and equivalence.
The withdrawal of cyclosporine and concurrent increases in sirolimus trough concentrations to steady-state required approximately 6 weeks. Larger Rapamune ® doses were required due to the absence of the inhibition of sirolimus metabolism and transport by cyclosporine and to achieve higher target concentrations during concentration-controlled administration following cyclosporine withdrawal.
Special Populations
Hepatic impairment: Sirolimus oral solution (15 mg) was administered as a single oral dose to 18 subjects with normal hepatic function and to 18 patients with Child-Pugh classification A or B hepatic impairment, in which hepatic impairment was primary and not related to an underlying systemic disease. Shown below are the mean ± SD pharmacokinetic parameters following the administration of sirolimus oral solution.
SIROLIMUS PHARMACOKINETIC PARAMETERS (MEAN ± SD) IN 18 HEALTHY SUBJECTS AND 18 PATIENTS WITH HEPATIC IMPAIRMENT (15 MG SINGLE DOSE - ORAL SOLUTION) PopulationC max,ss a
(ng/mL)t max
(h)AUC 0-(infinity)
(ng·h/mL)CL/F/WT
(mL/h/kg)Healthy subjects78.2 ± 18.3 0.82 ± 0.17 970 ± 272 215 ± 76 Hepatic impairment77.9 ± 23.1 0.84 ± 0.17 1567 ± 616 144 ± 62 a: As measured by LC/MS/MS.
Compared with the values in the normal hepatic group, the hepatic impairment group had higher mean values for sirolimus AUC (61%) and t 1/2 (43%) and had lower mean values for sirolimus CL/F/WT (33%). The mean t 1/2 increased from 79 ± 12 hours in subjects with normal hepatic function to 113 ± 41 hours in patients with impaired hepatic function. The rate of absorption of sirolimus was not altered by hepatic disease, as evidenced by C max and t max values. However, hepatic diseases with varying etiologies may show different effects and the pharmacokinetics of sirolimus in patients with severe hepatic dysfunction is unknown. Dosage adjustment is recommended for patients with mild to moderate hepatic impairment (see DOSAGE AND ADMINISTRATION ).
Renal impairment: The effect of renal impairment on the pharmacokinetics of sirolimus is not known. However, there is minimal (2.2%) renal excretion of the drug or its metabolites.
Pediatric: Sirolimus pharmacokinetic data were collected in concentration-controlled trials of pediatric renal transplant patients who were also receiving cyclosporine and corticosteroids. The target ranges for trough concentrations were either 10-20 ng/mL for the 21 children receiving tablets, or 5-15 ng/mL for the one child receiving oral solution. The children aged 6-11 years (n = 8) received mean ± SD doses of 1.75 ± 0.71 mg/day (0.064 ± 0.018 mg/kg, 1.65 ± 0.43 mg/m 2 ). The children aged 12-18 years (n = 14) received mean ± SD doses of 2.79 ± 1.25 mg/day (0.053 ± 0.0150 mg/kg, 1.86 ± 0.61 mg/m 2 ). At the time of sirolimus blood sampling for pharmacokinetic evaluation, the majority (80%) of these pediatric patients received the sirolimus dose at 16 hours after the once daily cyclosporine dose.
SIROLIMUS PHARMACOKINETIC PARAMETERS (MEAN ± SD) IN PEDIATRIC RENAL TRANSPLANT PATIENTS (MULTIPLE DOSE CONCENTRATION CONTROL) a , b Age
(y)n Body
weight
(kg)C max,ss
(ng/mL)t max,ss
(h)C min, ss
(ng/ml)AUC [tgr ],ss
(ng·h/mL)CL/F c
(mL/h/kg)CL/F c
(L/h/m 2 )6-11 8 27 ± 10 22.1 ± 8.9 5.88 ± 4.05 10.6 ± 4.3 356 ± 127 214 ± 129 5.4 ± 2.8 12-18 14 52 ± 15 34.5 ± 12.2 2.7 ± 1.5 14.7 ± 8.6 466 ± 236 136 ± 57 4.7 ± 1.9 a:Sirolimus co-administered with cyclosporine oral solution (MODIFIED) (e.g., Neoral Oral Solution) and/or cyclosporine capsules (MODIFIED) (e.g., Neoral Soft Gelatin Capsules). b:As measured by Liquid Chromatographic/Tandem Mass Spectrometric Method (LC/MS/MS). c:Oral-dose clearance adjusted by either body weight (kg) or body surface area (m 2 ).
The table below summarizes pharmacokinetic data obtained in pediatric dialysis patients with chronically impaired renal function.
SIROLIMUS PHARMACOKINETIC PARAMETERS (MEAN ± SD) IN PEDIATRIC PATIENTS WITH STABLE CHRONIC RENAL FAILURE MAINTAINED ON HEMODIALYSIS OR PERITONEAL DIALYSIS (1, 3, 9, 15 MG/M 2 SINGLE DOSE) * Age Group (y)n t max (h) t 1/2 (h) CL/F (mL/h/kg) 5-119 1.1 ± 0.5 71 ± 40 580 ± 450 12-1811 0.79 ± 0.17 55 ± 18 450 ± 232 * All subjects received sirolimus oral solutionGeriatric: Clinical studies of Rapamune did not include a sufficient number of patients >65 years of age to determine whether they will respond differently than younger patients. After the administration of Rapamune Oral Solution, sirolimus trough concentration data in 35 renal transplant patients >65 years of age were similar to those in the adult population (n = 822) 18 to 65 years of age. Similar results were obtained after the administration of Rapamune Tablets to 12 renal transplant patients >65 years of age compared with adults (n = 167) 18 to 65 years of age.
Gender: After the administration of Rapamune Oral Solution, sirolimus oral dose clearance in males was 12% lower than that in females; male subjects had a significantly longer t 1/2 than did female subjects (72.3 hours versus 61.3 hours). A similar trend in the effect of gender on sirolimus oral dose clearance and t 1/2 was observed after the administration of Rapamune Tablets. Dose adjustments based on gender are not recommended.
Race: In large phase 3 trials (Studies 1 and 2) using Rapamune Oral Solution and cyclosporine oral solution (MODIFIED) (e.g., Neoral ® Oral Solution) and/or cyclosporine capsules (MODIFIED) (e.g., Neoral ® Soft Gelatin Capsules), there were no significant differences in mean trough sirolimus concentrations over time between black (n = 139) and non-black (n = 724) patients during the first 6 months after transplantation at sirolimus doses of 2 mg/day and 5 mg/day. Similarly, after administration of Rapamune Tablets (2 mg/day) in a phase III trial, mean sirolimus trough concentrations over 6 months were not significantly different among black (n = 51) and non-black (n = 128) patients.
CLINICAL STUDIES
Rapamune ® Oral Solution: The safety and efficacy of Rapamune ® Oral Solution for the prevention of organ rejection following renal transplantation were assessed in two randomized, double-blind, multicenter, controlled trials. These studies compared two dose levels of Rapamune Oral Solution (2 mg and 5 mg, once daily) with azathioprine (Study 1) or placebo (Study 2) when administered in combination with cyclosporine and corticosteroids. Study 1 was conducted in the United States at 38 sites. Seven hundred nineteen (719) patients were enrolled in this trial and randomized following transplantation; 284 were randomized to receive Rapamune Oral Solution 2 mg/day, 274 were randomized to receive Rapamune Oral Solution 5 mg/day, and 161 to receive azathioprine 2-3 mg/kg/day. Study 2 was conducted in Australia, Canada, Europe, and the United States, at a total of 34 sites. Five hundred seventy-six (576) patients were enrolled in this trial and randomized before transplantation; 227 were randomized to receive Rapamune Oral Solution 2 mg/day, 219 were randomized to receive Rapamune Oral Solution 5 mg/day, and 130 to receive placebo. In both studies, the use of antilymphocyte antibody induction therapy was prohibited. In both studies, the primary efficacy endpoint was the rate of efficacy failure in the first 6 months after transplantation. Efficacy failure was defined as the first occurrence of an acute rejection episode (confirmed by biopsy), graft loss, or death.
The tables below summarize the results of the primary efficacy analyses from these trials. Rapamune Oral Solution, at doses of 2 mg/day and 5 mg/day, significantly reduced the incidence of efficacy failure (statistically significant at the <0.025 level; nominal significance level adjusted for multiple [2] dose comparisons) at 6 months following transplantation compared with both azathioprine and placebo.
INCIDENCE (%) OF EFFICACY FAILURE AT 6 AND 24 MONTHS FOR STUDY 1 a , b ParameterRapamune ®
Oral Solution
2 mg/day
(n = 284)Rapamune ®
Oral Solution
5 mg/day
(n = 274)Azathioprine
2-3 mg/kg/day
(n = 161)Efficacy failure at 6 months c18.7 16.8 32.3 Components of efficacy failureBiopsy-proven acute rejection16.5 11.3 29.2 Graft loss1.1 2.9 2.5 Death0.7 1.8 0 Lost to follow-up0.4 0.7 0.6 Efficacy failure at 24 months32.8 25.9 36.0 Components of efficacy failureBiopsy-proven acute rejection23.6 17.5 32.3 Graft loss3.9 4.7 3.1 Death4.2 3.3 0 Lost to follow-up1.1 0.4 0.6 a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.c: Primary endpoint.
INCIDENCE (%) OF EFFICACY FAILURE AT 6 AND 36 MONTHS FOR STUDY 2 a , b ParameterRapamune ®
Oral Solution
2 mg/day
(n = 227)Rapamune ®
Oral Solution
5 mg/day
(n = 219)Placebo
(n = 130)Efficacy failure at 6 months c30.0 25.6 47.7 Components of efficacy failureBiopsy-proven acute rejection24.7 19.2 41.5 Graft loss3.1 3.7 3.9 Death2.2 2.7 2.3 Lost to follow-up0 0 0 Efficacy failure at 36 months44.1 41.6 54.6 Components of efficacy failureBiopsy-proven acute rejection32.2 27.4 43.9 Graft loss6.2 7.3 4.6 Death5.7 5.9 5.4 Lost to follow-up0 0.9 0.8 a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.c: Primary endpoint.
Patient and graft survival at 1 year were co-primary endpoints. The table below shows graft and patient survival at 1 and 2 years in Study 1 and 1 and 3 years in Study 2. The graft and patient survival rates were similar in patients treated with Rapamune and comparator-treated patients.
GRAFT AND PATIENT SURVIVAL (%) FOR STUDY 1 (12 AND 24 MONTHS) AND STUDY 2 (12 AND 36 MONTHS) a , b ParameterRapamune ®
Oral Solution
2 mg/dayRapamune ®
Oral Solution
5 mg/dayAzathioprine
2-3 mg/kg/dayPlacebo Study 1(n = 284) (n = 274) (n = 161) Graft survivalMonth 1294.7 92.7 93.8 Month 2485.2 89.1 90.1 Patient survivalMonth 1297.2 96.0 98.1 Month 2492.6 94.9 96.3 Study 2(n = 227) (n = 219) (n = 130) Graft survivalMonth 1289.9 90.9 87.7 Month 3681.1 79.9 80.8 Patient survivalMonth 1296.5 95.0 94.6 Month 3690.3 89.5 90.8 a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.
The reduction in the incidence of first biopsy-confirmed acute rejection episodes in patients treated with Rapamune compared with the control groups included a reduction in all grades of rejection.
In Study 1, which was prospectively stratified by race within center, efficacy failure was similar for Rapamune Oral Solution 2 mg/day and lower for Rapamune Oral Solution 5 mg/day compared with azathioprine in black patients. In Study 2, which was not prospectively stratified by race, efficacy failure was similar for both Rapamune Oral Solution doses compared with placebo in black patients. The decision to use the higher dose of Rapamune Oral Solution in black patients must be weighed against the increased risk of dose-dependent adverse events that were observed with the Rapamune Oral Solution 5-mg dose (see ADVERSE REACTIONS ).
PERCENTAGE OF EFFICACY FAILURE BY RACE AT 6 MONTHS a , b ParameterRapamune ®
Oral Solution
2 mg/dayRapamune ®
Oral Solution
5 mg/dayAzathioprine
2-3 mg/kg/dayPlacebo Study 1Black (n = 166)34.9 (n = 63) 18.0 (n = 61) 33.3 (n = 42) Non-black (n = 553)14.0 (n = 221) 16.4 (n = 213) 31.9 (n = 119) Study 2Black (n = 66)30.8 (n = 26) 33.7 (n = 27) 38.5 (n = 13) Non-black (n = 510)29.9 (n = 201) 24.5 (n = 192) 48.7 (n = 117) a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.
Mean glomerular filtration rates (GFR) post transplant were calculated by using the Nankivell equation at 12 and 24 months for Study 1, and 12 and 36 months for Study 2. Mean GFR was lower in patients treated with cyclosporine and Rapamune Oral Solution compared with those treated with cyclosporine and the respective azathioprine or placebo control.
OVERALL CALCULATED GLOMERULAR FILTRATION RATES (Mean ± SEM, cc/min)
BY NANKIVELL EQUATION POST TRANSPLANT a , bParameterRapamune ®
Oral Solution
2 mg/dayRapamune ®
Oral Solution
5 mg/dayAzathioprine
2-3 mg/kg/dayPlacebo Study 1Month 1257.4 ± 1.3
(n = 269)54.6 ± 1.3
(n = 248)64.1 ± 1.6
(n = 149)Month 2458.4 ± 1.5
(n = 221)52.6 ± 1.5
(n = 222)62.4 ± 1.9
(n = 132)Study 2Month 1252.4 ± 1.5
(n = 211)51.5 ± 1.5
(n = 199)58.0 ± 2.1
(n = 117)Month 3648.1 ± 1.8
(n = 183)46.1 ± 2.0
(n = 177)53.4 ± 2.7
(n = 102)a: Includes patients who prematurely discontinued treatment.b: Patients who had a graft loss were included in the analysis with GFR set to 0.0.
Within each treatment group in Studies 1 and 2, mean GFR at one year post transplant was lower in patients who experienced at least 1 episode of biopsy-proven acute rejection, compared with those who did not.
Renal function should be monitored and appropriate adjustment of the immunosuppression regimen should be considered in patients with elevated or increasing serum creatinine levels (see PRECAUTIONS ).
Rapamune ® Tablets: The safety and efficacy of Rapamune Oral Solution and Rapamune Tablets for the prevention of organ rejection following renal transplantation were compared in a randomized multicenter controlled trial (Study 3). This study compared a single dose level (2 mg, once daily) of Rapamune Oral Solution and Rapamune Tablets when administered in combination with cyclosporine and corticosteroids. The study was conducted at 30 centers in Australia, Canada, and the United States. Four hundred seventy-seven (477) patients were enrolled in this study and randomized before transplantation; 238 patients were randomized to receive Rapamune Oral Solution 2 mg/day and 239 patients were randomized to receive Rapamune Tablets 2 mg/day. In this study, the use of antilymphocyte antibody induction therapy was prohibited. The primary efficacy endpoint was the rate of efficacy failure in the first 3 months after transplantation. Efficacy failure was defined as the first occurrence of an acute rejection episode (confirmed by biopsy), graft loss, or death.
The table below summarizes the result of the efficacy failure analysis at 3 and 6 months from this trial. The overall rate of efficacy failure at 3 months, the primary endpoint, in the tablet treatment group was equivalent to the rate in the oral solution treatment group.
INCIDENCE (%) OF EFFICACY FAILURE AT 3 AND 6 MONTHS: STUDY 3 a , b Rapamune ®
Oral Solution
(n = 238)Rapamune ®
Tablets
(n = 239)Efficacy Failure at 3 months c23.5 24.7 Components of efficacy failureBiopsy-proven acute rejection18.9 17.6 Graft loss3.4 6.3 Death1.3 0.8 Efficacy Failure at 6 months26.1 27.2 Components of efficacy failureBiopsy-proven acute rejection21.0 19.2 Graft loss3.4 6.3 Death1.7 1.7 a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.c: Efficacy failure at 3 months was the primary endpoint.
Graft and patient survival at 12 months were co-primary endpoints. There was no significant difference between the oral solution and tablet formulations for both graft and patient survival. Graft survival was 92.0% and 88.7% for the oral solution and tablet treatment groups, respectively. The patient survival rates in the oral solution and tablet treatment groups were 95.8% and 96.2%, respectively.
The mean GFR at 12 months, calculated by the Nankivell equation, were not significantly different for the oral solution group and for the tablet group.
The table below summarizes the mean GFR at one-year post-transplantation for all patients in Study 3 who had serum creatinine measured at 12 months.
OVERALL CALCULATED GLOMERULAR FILTRATION
RATES (CC/MIN) BY NANKIVELL EQUATION AT
12 MONTHS POST TRANSPLANT: STUDY 3 a , bRapamune ®
Oral SolutionRapamune ®
TabletsMean ± SEM 53.1 ± 1.7
(n = 229)51.7 ± 1.7
(n = 225)a: Includes patients who prematurely discontinued treatment. b: Patients who had a graft loss were included in the analysis with GFR set to 0.0.
In Study 4, the safety and efficacy of Rapamune as a maintenance regimen were assessed following cyclosporine withdrawal at 3 to 4 months post renal transplantation. Study 4 was a randomized, multicenter, controlled trial conducted at 57 centers in Australia, Canada, and Europe. Five hundred twenty-five (525) patients were enrolled. All patients in this study received the tablet formulation. This study compared patients who were administered Rapamune, cyclosporine, and corticosteroids continuously with patients who received the same standardized therapy for the first 3 months after transplantation (prerandomization period) followed by the withdrawal of cyclosporine. During cyclosporine withdrawal the Rapamune dosages were adjusted to achieve targeted sirolimus whole blood trough concentration ranges (20 to 30 ng/mL, experimental immunoassay). At 3 months, 430 patients were equally randomized to either Rapamune with cyclosporine therapy or Rapamune as a maintenance regimen following cyclosporine withdrawal. Eligibility for randomization included no Banff Grade 3 acute rejection episode or vascular rejection in the 4 weeks before random assignment; serum creatinine </= 4.5 mg/dL; and adequate renal function to support cyclosporine withdrawal (in the opinion of the investigator). The primary efficacy endpoint was graft survival at 12 months after transplantation. Secondary efficacy endpoints were the rate of biopsy-confirmed acute rejection, patient survival, incidence of efficacy failure (defined as the first occurrence of either biopsy-proven acute rejection, graft loss, or death), and treatment failure (defined as the first occurrence of either discontinuation, acute rejection, graft loss, or death).
The safety and efficacy of cyclosporine withdrawal in high-risk patients have not been adequately studied and it is therefore not recommended. This includes patients with Banff grade III acute rejection or vascular rejection prior to cyclosporine withdrawal, those who are dialysis-dependent, serum creatinine > 4.5 mg/dL, black patients, re-transplants, multi-organ transplants, or patients with high panel of reactive antibodies (See INDICATIONS AND USAGE ).
The table below summarizes the resulting graft and patient survival at 12, 24, and 36 months for this trial. At 12, 24, and 36 months, graft and patient survival were similar for both groups.
GRAFT AND PATIENT SURVIVAL (%): STUDY 4 a ParameterRapamune with Cyclosporine Therapy (n = 215) Rapamune Following Cyclosporine Withdrawal (n = 215) Graft SurvivalMonth 12 b95.8 97.2 Month 2491.2 93.5 Month 3685.1 91.2 Patient SurvivalMonth 1297.2 98.1 Month 2494.0 95.3 Month 3688.4 93.5 a: Includes patients who prematurely discontinued treatment.b: Primary efficacy endpoint.
The table below summarizes the results of first biopsy-proven acute rejection at 12 and 36 months. There was a significant difference in first biopsy-proven rejection between the two groups during post-randomization through 12 months. Most of the post-randomization acute rejections occurred in the first 3 months following randomization.
INCIDENCE OF FIRST BIOPSY-PROVEN
ACUTE REJECTION (%) BY TREATMENT GROUP AT
36 MONTHS: STUDY 4 aPeriodRapamune with Cyclosporine
Therapy (n = 215)Rapamune Following
Cyclosporine withdrawal
(n = 215)Prerandomization b9.3 10.2 Postrandomization
through 12 months b4.2 9.8 Postrandomization
from 12 to 36 months1.4 0.5 Postrandomization
through 36 months5.6 10.2 Total at 36 months14.9 20.5 a: Includes patients who prematurely discontinued treatment.b: Randomization occurred at 3 months ± 2 weeks.
Patients receiving renal allografts with >/= 4 HLA mismatches experienced significantly higher rates of acute rejection following randomization to the cyclosporine withdrawal group compared with patients who continued cyclosporine (15.3% vs 3.0%). Patients receiving renal allografts with </= 3 HLA mismatches, demonstrated similar rates of acute rejection between treatment groups (6.8% vs 7.7%) following randomization.
The table below summarizes the mean calculated GFR in Study 4.
CALCULATED GLOMERULAR FILTRATION RATES
(mL/min) BY NANKIVELL EQUATION AT 12, 24,
AND 36 MONTHS POST TRANSPLANT: STUDY 4 a , bParameterRapamune with
Cyclosporine TherapyRapamune Following
Cyclosporine WithdrawalMonth 12Mean ± SEM53.2 ± 1.5
n = 20859.3 ± 1.5
n = 203Month 24Mean ± SEM48.4 ± 1.7
n = 20358.4 ± 1.6
n = 201Month 36Mean ± SEM47.3 ± 1.8
(n = 194)59.4 ± 1.8
(n = 194)a: Includes patients who prematurely discontinued treatment.b: Patients who had a graft loss were included in the analysis and had their GFR set to 0.0.
The mean GFR at 12, 24, and 36 months, calculated by the Nankivell equation, was significantly higher for patients receiving Rapamune as a maintenance regimen following cyclosporine withdrawal than for those in the Rapamune with cyclosporine therapy group. Patients who had an acute rejection prior to randomization had a significantly higher GFR following cyclosporine withdrawal compared to those in the Rapamune with cyclosporine group. There was no significant difference in GFR between groups for patients who experienced acute rejection postrandomization.
Pediatrics: Rapamune ® was evaluated in a 36-month, open-label, randomized, controlled clinical trial at 14 North American centers in pediatric (aged 3 to < 18 years) renal transplant recipients considered to be at high immunologic risk for developing chronic allograft nephropathy, defined as a history of one or more acute allograft rejection episodes and/or the presence of chronic allograft nephropathy on a renal biopsy. Seventy-eight (78) subjects were randomized in a 2:1 ratio to Rapamune ® (sirolimus target concentrations of 5 to 15 ng/mL, by chromatographic assay, n = 53) in combination with a calcineurin inhibitor and corticosteroids or to continue calcineurin-inhibitor-based immunosuppressive therapy (n = 25). The primary endpoint of the study was efficacy failure as defined by the first occurrence of biopsy confirmed acute rejection, graft loss, or death, and the trial was designed to show superiority of Rapamune ® added to a calcineurin-inhibitor-based immunosuppressive regimen compared to a calcineurin-inhibitor-based regimen. The cumulative incidence of efficacy failure up to 36 months was 45.3% in the Rapamune ® group compared to 44.0% in the control group, and did not demonstrate superiority. There was one death in each group. The use of Rapamune ® in combination with calcineurin inhibitors and corticosteroids was associated with an increased risk of deterioration of renal function, serum lipid abnormalities (including but not limited to increased serum triglycerides and cholesterol), and urinary tract infections. This study does not support the addition of Rapamune ® to calcineurin-inhibitor-based immunosuppressive therapy in this subpopulation of pediatric renal transplant patients.
INDICATIONS AND USAGE
Rapamune ® (sirolimus) is indicated for the prophylaxis of organ rejection in patients aged 13 years or older receiving renal transplants. It is recommended that Rapamune be used initially in a regimen with cyclosporine and corticosteroids. In patients at low to moderate immunologic risk cyclosporine should be withdrawn 2 to 4 months after transplantation and Rapamune ® dose should be increased to reach recommended blood concentrations (See DOSAGE AND ADMINISTRATION ).
The safety and efficacy of cyclosporine withdrawal in high-risk patients have not been adequately studied and it is therefore not recommended. This includes patients with Banff grade III acute rejection or vascular rejection prior to cyclosporine withdrawal, those who are dialysis-dependent, or with serum creatinine > 4.5 mg/dL, black patients, re-transplants, multi-organ transplants, patients with high panel of reactive antibodies (See CLINICAL STUDIES ).
The safety and efficacy of Rapamune ® have not been established in pediatric patients less than 13 years old, or in pediatric (< 18 years) renal transplant recipients considered at high immunologic risk (see PRECAUTIONS , Pediatric use , and CLINICAL STUDIES , Pediatrics ).
CONTRAINDICATIONS
Rapamune is contraindicated in patients with a hypersensitivity to sirolimus or its derivatives or any component of the drug product.
WARNINGS
Increased susceptibility to infection and the possible development of lymphoma and other malignancies, particularly of the skin, may result from immunosuppression (see ADVERSE REACTIONS ). Oversuppression of the immune system can also increase susceptibility to infection including opportunistic infections, fatal infections, and sepsis. Only physicians experienced in immunosuppressive therapy and management of organ transplant patients should use Rapamune. Patients receiving the drug should be managed in facilities equipped and staffed with adequate laboratory and supportive medical resources. The physician responsible for maintenance therapy should have complete information requisite for the follow-up of the patient.
Hypersensitivity reactions, including anaphylactic/anaphylactoid reactions, have been associated with the administration of sirolimus (see ADVERSE REACTIONS ).
As usual for patients with increased risk for skin cancer, exposure to sunlight and UV light should be limited by wearing protective clothing and using a sunscreen with a high protection factor.
Increased serum cholesterol and triglycerides, that may require treatment, occurred more frequently in patients treated with Rapamune compared with azathioprine or placebo controls (see PRECAUTIONS ).
In Studies 1 and 2, from month 6 through months 24 and 36, respectively, mean serum creatinine was increased and mean glomerular filtration rate was decreased in patients treated with Rapamune and cyclosporine compared with those treated with cyclosporine and placebo or azathioprine controls. The rate of decline in renal function was greater in patients receiving Rapamune and cyclosporine compared with control therapies (see CLINICAL STUDIES ).
Renal function should be closely monitored during the administration of Rapamune ® in combination with cyclosporine since long-term administration can be associated with deterioration of renal function. Appropriate adjustment of the immunosuppression regimen, including discontinuation of Rapamune and/or cyclosporine, should be considered in patients with elevated or increasing serum creatinine levels. Caution should be exercised when using other drugs which are known to impair renal function. In patients at low to moderate immunologic risk continuation of combination therapy with cyclosporine beyond 4 months following transplantation should only be considered when the benefits outweigh the risks of this combination for the individual patients (see PRECAUTIONS ).
In clinical trials, Rapamune has been administered concurrently with corticosteroids and with the following formulations of cyclosporine:
Sandimmune ® Injection (cyclosporine injection)
Sandimmune ® Oral Solution (cyclosporine oral solution)
Sandimmune ® Soft Gelatin Capsules (cyclosporine capsules)
Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED])
Neoral ® Oral Solution (cyclosporine oral solution [MODIFIED])
The efficacy and safety of the use of Rapamune in combination with other immunosuppressive agents has not been determined.
Liver Transplantation - Excess Mortality, Graft Loss, and Hepatic Artery Thrombosis (HAT):
The use of sirolimus in combination with tacrolimus was associated with excess mortality and graft loss in a study in de novo liver transplant recipients. Many of these patients had evidence of infection at or near the time of death.
In this and another study in de novo liver transplant recipients, the use of sirolimus in combination with cyclosporine or tacrolimus was associated with an increase in HAT; most cases of HAT occurred within 30 days post-transplantation and most led to graft loss or death.
Lung Transplantation - Bronchial Anastomotic Dehiscence:
Cases of bronchial anastomotic dehiscence, most fatal, have been reported in de novo lung transplant patients when sirolimus has been used as part of an immunosuppressive regimen.
The safety and efficacy of Rapamune ® (sirolimus) as immunosuppressive therapy have not been established in liver or lung transplant patients, and therefore, such use is not recommended.
Co-administration of sirolimus with strong inhibitors of CYP3A4 and/or P-gp (such as ketoconazole, voriconazole, itraconazole, erythromycin, telithromycin, or clarithromycin) or strong inducers of CYP3A4 and/or P-gp (such as rifampin or rifabutin) is not recommended (see CLINICAL PHARMACOLOGY , Metabolism , and PRECAUTIONS , Drug Interactions and Other drug interactions ).
PRECAUTIONS
General
Rapamune is intended for oral administration only.
Lymphocele, a known surgical complication of renal transplantation, occurred significantly more often in a dose-related fashion in patients treated with Rapamune. Appropriate operative measures should be considered to minimize this complication.
Lipids
The use of Rapamune ® in renal transplant patients was associated with increased serum cholesterol and triglycerides that may require treatment.
In Studies 1 and 2, in de novo renal transplant recipients who began the study with normal, fasting, total serum cholesterol (<200 mg/dL) or normal, fasting, total serum tri-glycerides (<200 mg/dL), there was an increased incidence of hypercholesterolemia (fasting serum cholesterol >240 mg/dL) or hypertriglyceridemia (fasting serum triglycerides >500 mg/dL), respectively, in patients receiving both Rapamune ® 2 mg and Rapamune ® 5 mg compared with azathioprine and placebo controls.
Treatment of new-onset hypercholesterolemia with lipid-lowering agents was required in 42-52% of patients enrolled in the Rapamune arms of Studies 1 and 2 compared with 16% of patients in the placebo arm and 22% of patients in the azathioprine arm.
In Study 4 during the prerandomization period, mean fasting serum cholesterol and triglyceride values rapidly increased, and peaked at 2 months with mean cholesterol values > 240 mg/dL and triglycerides > 250 mg/dL. After randomization mean cholesterol and triglyceride values remained higher in the cyclosporine withdrawal arm compared to the Rapamune ® and cyclosporine combination.
Renal transplant patients have a higher prevalence of clinically significant hyperlipidemia. Accordingly, the risk/benefit should be carefully considered in patients with established hyperlipidemia before initiating an immunosuppressive regimen including Rapamune.
Any patient who is administered Rapamune should be monitored for hyperlipidemia using laboratory tests and if hyperlipidemia is detected, subsequent interventions such as diet, exercise, and lipid-lowering agents, as outlined by the National Cholesterol Education Program guidelines, should be initiated.
In clinical trials, the concomitant administration of Rapamune and HMG-CoA reductase inhibitors and/or fibrates appeared to be well tolerated.
During Rapamune therapy with cyclosporine, patients administered an HMG-CoA reductase inhibitor and/or fibrate should be monitored for the possible development of rhabdomyolysis and other adverse effects as described in the respective labeling for these agents.
Renal Function
Patients treated with cyclosporine and Rapamune were noted to have higher serum creatinine levels and lower glomerular filtration rates compared with patients treated with cyclosporine and placebo or azathioprine controls (Studies 1 and 2). The rate of decline in renal function in these studies was greater in patients receiving Rapamune and cyclosporine compared with control therapies. In patients at low to moderate immunologic risk (See CLINICAL STUDIES ) continuation of combination therapy with cyclosporine beyond 4 months following transplantation should only be considered when the benefits outweigh the risks of this combination for the individual patients. (see WARNINGS ).
Renal function should be monitored during the administration of Rapamune ® in combination with cyclosporine. Appropriate adjustment of the immunosuppression regimen, including discontinuation of Rapamune and/or cyclosporine, should be considered in patients with elevated or increasing serum creatinine levels. Caution should be exercised when using agents (e.g., aminoglycosides, and amphotericin B) that are known to have a deleterious effect on renal function.
Antimicrobial Prophylaxis
Cases of Pneumocystis carinii pneumonia have been reported in patients not receiving antimicrobial prophylaxis. Therefore, antimicrobial prophylaxis for Pneumocystis carinii pneumonia should be administered for 1 year following transplantation.
Cytomegalovirus (CMV) prophylaxis is recommended for 3 months after transplantation, particularly for patients at increased risk for CMV disease.
Interstitial Lung Disease
Cases of interstitial lung disease (including pneumonitis, and infrequently bronchiolitis obliterans organizing pneumonia [BOOP] and pulmonary fibrosis), some fatal, with no identified infectious etiology have occurred in patients receiving immunosuppressive regimens including Rapamune. In some cases, the interstitial lung disease has resolved upon discontinuation or dose reduction of Rapamune. The risk may be increased as the trough Rapamune concentration increases (see ADVERSE REACTIONS, Other clinical experience ).
Information for Patients
Patients should be given complete dosage instructions (see PATIENT INSTRUCTIONS ). Women of childbearing potential should be informed of the potential risks during pregnancy and that they should use effective contraception prior to initiation of Rapamune therapy, during Rapamune therapy and for 12 weeks after Rapamune therapy has been stopped (see PRECAUTIONS : Pregnancy ).
Patients should be told that exposure to sunlight and UV light should be limited by wearing protective clothing and using a sunscreen with a high protection factor because of the increased risk for skin cancer (see WARNINGS ).
Laboratory Tests
Whole blood sirolimus concentrations should be monitored in patients receiving concentration-controlled Rapamune. Monitoring is also necessary in patients likely to have altered drug metabolism, in patients >/=13 years who weigh less than 40 kg, in patients with hepatic impairment, and during concurrent administration of potent CYP3A4 in-ducers and inhibitors (see PRECAUTIONS : Drug Interactions ).
Drug Interactions
Sirolimus is known to be a substrate for both cytochrome CYP3A4 and P-gp. The pharmacokinetic interaction between sirolimus and concomitantly administered drugs is discussed below. Drug interaction studies have not been conducted with drugs other than those described below.
Cyclosporine capsules MODIFIED:
Cyclosporine is a substrate and inhibitor of CYP3A4 and P-gp.
Because of the effect of cyclosporine capsules (MODIFIED), it is recommended that sirolimus should be taken 4 hours after administration of cyclosporine oral solution (MODIFIED) and/or cyclosporine capsules (MODIFIED) (see DOSAGE AND ADMINISTRATION ).
Studies assessing the effect of concomitant administration of cyclosporine capsules (MODIFIED) with sirolimus oral solution and with sirolimus tablets are summarized below.
Rapamune Oral Solution: In a single dose drug-drug interaction study, 24 healthy volunteers were administered 10 mg sirolimus either simultaneously or 4 hours after a 300 mg dose of Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]). For simultaneous administration, the mean C max and AUC of sirolimus were increased by 116% and 230%, respectively, relative to administration of sirolimus alone. However, when given 4 hours after Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]) administration, sirolimus C max and AUC were increased by 37% and 80%, respectively, compared with administration of sirolimus alone.
In a single-dose cross-over drug-drug interaction study, 33 healthy volunteers received 5 mg sirolimus alone, 2 hours before, and 2 hours after a 300 mg dose of Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]). When given 2 hours before Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]) administration, sirolimus C max and AUC were comparable to those with administration of sirolimus alone. However, when given 2 hours after, the mean C max and AUC of sirolimus were increased by 126% and 141%, respectively, relative to administration of sirolimus alone.
Mean cyclosporine C max and AUC were not significantly affected when sirolimus was given simultaneously or when administered 4 hours after Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]). However, after multiple-dose administration of sirolimus given 4 hours after Neoral ® in renal post-transplant patients over 6 months, cyclosporine oral-dose clearance was reduced, and lower doses of Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]) were needed to maintain target cyclosporine concentration.
Rapamune Tablets: In a single-dose drug-drug interaction study, 24 healthy volunteers were administered 10 mg sirolimus (Rapamune Tablets) either simultaneously or 4 hours after a 300-mg dose of Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]). For simultaneous administration, mean C max and AUC were increased by 512% and 148%, respectively, relative to administration of sirolimus alone. However, when given 4 hours after cyclosporine administration, sirolimus C max and AUC were both increased by only 33% compared with administration of sirolimus alone.
Cyclosporine oral solution: In a multiple-dose study in 150 psoriasis patients, sirolimus 0.5, 1.5, and 3 mg/m 2 /day was administered simultaneously with Sandimmune ® Oral Solution (cyclosporine Oral Solution) 1.25 mg/kg/day. The increase in average sirolimus trough concentrations ranged between 67% to 86% relative to when sirolimus was administered without cyclosporine. The intersubject variability (%CV) for sirolimus trough concentrations ranged from 39.7% to 68.7%. There was no significant effect of multiple-dose sirolimus on cyclosporine trough concentrations following Sandimmune ® Oral Solution (cyclosporine oral solution) administration. However, the %CV was higher (range 85.9%-165%) than those from previous studies.
Sandimmune ® Oral Solution (cyclosporine oral solution) is not bioequivalent to Neoral ® Oral Solution (cyclosporine oral solution MODIFIED), and should not be used interchangeably. Although there is no published data comparing Sandimmune ® Oral Solution (cyclosporine oral solution) to SangCya ® Oral Solution (cyclosporine oral solution [MODIFIED]), they should not be used interchangeably. Likewise, Sandimmune ® Soft Gelatin Capsules (cyclosporine capsules) are not bioequivalent to Neoral ® Soft Gelatin Capsules (cyclosporine capsules [MODIFIED]) and should not be used interchangeably.
Diltiazem: Diltiazem is a substrate and inhibitor of CYP3A4 and P-gp; sirolimus concentrations should be monitored and a dose adjustment may be necessary. The simultaneous oral administration of 10 mg of sirolimus oral solution and 120 mg of diltiazem to 18 healthy volunteers significantly affected the bioavailability of sirolimus. Sirolimus C max , t max , and AUC were increased 1.4-, 1.3-, and 1.6-fold, respectively. Sirolimus did not affect the pharmacokinetics of either diltiazem or its metabolites desacetyldiltiazem and desmethyldiltiazem.
Erythromycin: Erythromycin is a substrate and inhibitor of CYP3A4 and P-gp; co-administration of sirolimus oral solution or tablets and erythromycin is not recommended (see WARNINGS ). The simultaneous oral administration of 2 mg daily of sirolimus oral solution and 800 mg q 8h of erythromycin as erythromycin ethylsuccinate tablets at steady state to 24 healthy volunteers significantly affected the bioavailability of sirolimus and erythromycin. Sirolimus C max and AUC were increased 4.4- and 4.2-fold respectively and t max was increased by 0.4 hr. Erythromycin C max and AUC were increased 1.6- and 1.7-fold, respectively, and t max was increased by 0.3 hr.
Ketoconazole: Ketoconazole is a strong inhibitor of CYP3A4 and P-gp; co-administration of sirolimus oral solution or tablets and ketoconazole is not recommended (see WARNINGS ). Multiple-dose ketoconazole administration significantly affected the rate and extent of absorption and sirolimus exposure after administration of Rapamune ® Oral Solution, as reflected by increases in sirolimus C max , t max , and AUC of 4.3-fold, 38%, and 10.9-fold, respectively. However, the terminal t 1/2 of sirolimus was not changed. Single-dose sirolimus did not affect steady-state 12-hour plasma ketoconazole concentrations.
Rifampin: Rifampin is a strong inducer of CYP3A4 and P-gp; co-administration of sirolimus oral solution or tablets and rifampin is not recommended (see WARNINGS ). Pretreatment of 14 healthy volunteers with multiple doses of rifampin, 600 mg daily for 14 days, followed by a single 20-mg dose of sirolimus oral solution, greatly increased sirolimus oral-dose clearance by 5.5-fold (range = 2.8 to 10), which represents mean decreases in AUC and C max of about 82% and 71%, respectively. In patients where rifampin is indicated, alternative therapeutic agents with less enzyme induction potential should be considered.
Verapamil: Verapamil is a substrate and inhibitor of CYP3A4 and P-gp; sirolimus concentrations should be monitored and a dose adjustment may be necessary. The simultaneous oral administration of 2 mg daily of sirolimus oral solution and 180 mg q 12h of verapamil at steady state to 26 healthy volunteers significantly affected the bioavailability of sirolimus and verapamil. Sirolimus C max and AUC were increased 2.3- and 2.2-fold, respectively, without substantial change in t max . The C max and AUC of the pharmacologically active S(-) enantiomer of verapamil were both increased 1.5-fold and t max was decreased by 1.2 hr.
Drugs which may be coadministered without dose adjustment
Clinically significant pharmacokinetic drug-drug interactions were not observed in studies of drugs listed below. A synopsis of the type of study performed for each drug is provided. Sirolimus and these drugs may be coadministered without dose adjustments.
Acyclovir: Acyclovir, 200 mg, was administered once daily for 3 days followed by a single 10-mg dose of sirolimus oral solution on day 3 in 20 adult healthy volunteers.
Digoxin: Digoxin, 0.25 mg, was administered daily for 8 days and a single 10-mg dose of sirolimus oral solution was given on day 8 to 24 healthy volunteers.
Glyburide: A single 5-mg dose of glyburide and a single 10-mg dose of sirolimus oral solution were administered to 24 healthy volunteers. Sirolimus did not affect the hypoglycemic action of glyburide.
Nifedipine: A single 60-mg dose of nifedipine and a single 10-mg dose of sirolimus oral solution were administered to 24 healthy volunteers.
Norgestrel/ethinyl estradiol (Lo/Ovral ® ): Sirolimus oral solution, 2 mg, was given daily for 7 days to 21 healthy female volunteers on norgestrel/ethinyl estradiol.
Prednisolone: Pharmacokinetic information was obtained from 42 stable renal transplant patients receiving daily doses of prednisone (5-20 mg/day) and either single or multiple doses of sirolimus oral solution (0.5-5 mg/m 2 q 12h).
Sulfamethoxazole/trimethoprim (Bactrim ® ): A single oral dose of sulfamethoxazole (400 mg)/trimethoprim (80 mg) was given to 15 renal transplant patients receiving daily oral doses of sirolimus (8 to 25 mg/m 2 ).
Other drug interactions
Co-administration of sirolimus with strong inhibitors of CYP3A4 and/or P-gp (such as ketoconazole, voriconazole, itraconazole, erythromycin, telithromycin, or clarithromycin) or strong inducers of CYP3A4 and/or P-gp (such as rifampin or rifabutin) is not recommended (see WARNINGS ). Sirolimus is extensively metabolized by the CYP3A4 isoenzyme in the intestinal wall and liver and undergoes counter-transport from enterocytes of the small intestine into the gut lumen by the P-gp drug efflux pump. Sirolimus is potentially recycled between enterocytes and the gut lumen to allow continued metabolism by CYP3A4. Therefore, absorption and the subsequent elimination of systemically absorbed sirolimus may be influenced by drugs that affect these proteins. Strong inhibitors of CYP3A4 and P-gp significantly decrease the metabolism of sirolimus and increase sirolimus concentrations, while strong inducers of CYP3A4 and P-gp significantly increase the metabolism of sirolimus and decrease sirolimus concentrations.
In patients in whom strong inhibitors or inducers of CYP3A4 are indicated, alternative therapeutic agents with less potential for inhibition or induction of CYP3A4 should be considered.
Sirolimus is a substrate for the multidrug efflux pump, P-gp in the small intestine. Therefore, absorption of sirolimus may be influenced by drugs that affect P-gp.
Aside from those mentioned above, other drugs that increase sirolimus blood concentrations include (but are not limited to):
Calcium channel blockers: nicardipine.
Antifungal agents: clotrimazole, fluconazole.
Antibiotics: troleandomycin.
Gastrointestinal prokinetic agents: cisapride, metoclopramide.
Other drugs: bromocriptine, cimetidine, danazol, HIV- protease inhibitors (e.g., ritonavir, indinavir).
Aside from those mentioned above, other drugs that decrease sirolimus concentrations include (but are not limited to):
Anticonvulsants: carbamazepine, phenobarbital, phenytoin.
Antibiotics: rifapentine.
Care should be exercised when drugs or other substances that are metabolized by CYP3A4 are administered concomitantly with Rapamune. Grapefruit juice reduces CYP3A4-mediated metabolism of Rapamune and must not be used for dilution (see DOSAGE AND ADMINISTRATION ).
Herbal Preparations
St. John's Wort ( hypericum perforatum ) induces CYP3A4 and P-gp. Since sirolimus is a substrate for both cytochrome CYP3A4 and P-gp, there is the potential that the use of St. John's Wort in patients receiving Rapamune could result in reduced sirolimus concentrations.
Vaccination
Immunosuppressants may affect response to vaccination. Therefore, during treatment with Rapamune, vaccination may be less effective. The use of live vaccines should be avoided; live vaccines may include, but are not limited to measles, mumps, rubella, oral polio, BCG, yellow fever, varicella, and TY21a typhoid.
Drug-Laboratory Test Interactions
There are no studies on the interactions of sirolimus in commonly employed clinical laboratory tests.
Carcinogenesis, Mutagenesis, and Impairment of Fertility
Sirolimus was not genotoxic in the in vitro bacterial reverse mutation assay, the Chinese hamster ovary cell chromosomal aberration assay, the mouse lymphoma cell forward mutation assay, or the in vivo mouse micronucleus assay.
Carcinogenicity studies were conducted in mice and rats. In an 86-week female mouse study at dosages of 0, 12.5, 25 and 50/6 (dosage lowered from 50 to 6 mg/kg/day at week 31 due to infection secondary to immunosuppression) there was a statistically significant increase in malignant lymphoma at all dose levels (approximately 16 to 135 times the clinical doses adjusted for body surface area) compared with controls. In a second mouse study at dosages of 0, 1, 3 and 6 mg/kg (approximately 3 to 16 times the clinical dose adjusted for body surface area), hepatocellular adenoma and carcinoma (males), were considered Rapamune related. In the 104-week rat study at dosages of 0, 0.05, 0.1, and 0.2 mg/kg/day (approximately 0.4 to 1 times the clinical dose adjusted for body surface area), there was a statistically significant increased incidence of testicular adenoma in the 0.2 mg/kg/day group.
There was no effect on fertility in female rats following the administration of sirolimus at dosages up to 0.5 mg/kg (approximately 1 to 3 times the clinical doses adjusted for body surface area). In male rats, there was no significant difference in fertility rate compared to controls at a dosage of 2 mg/kg (approximately 4 to 11 times the clinical doses adjusted for body surface area). Reductions in testicular weights and/or histological lesions (e.g., tubular atrophy and tubular giant cells) were observed in rats following dosages of 0.65 mg/kg (approximately 1 to 3 times the clinical doses adjusted for body surface area) and above and in a monkey study at 0.1 mg/kg (approximately 0.4 to 1 times the clinical doses adjusted for body surface area) and above. Sperm counts were reduced in male rats following the administration of sirolimus for 13 weeks at a dosage of 6 mg/kg (approximately 12 to 32 times the clinical doses adjusted for body surface area), but showed improvement by 3 months after dosing was stopped.
Pregnancy
Pregnancy Category C: Sirolimus was embryo/feto toxic in rats at dosages of 0.1 mg/kg and above (approximately 0.2 to 0.5 the clinical doses adjusted for body surface area). Embryo/feto toxicity was manifested as mortality and reduced fetal weights (with associated delays in skeletal ossification). However, no teratogenesis was evident. In combination with cyclosporine, rats had increased embryo/feto mortality compared with Rapamune alone. There were no effects on rabbit development at the maternally toxic dosage of 0.05 mg/kg (approximately 0.3 to 0.8 times the clinical doses adjusted for body surface area). There are no adequate and well controlled studies in pregnant women. Effective contraception must be initiated before Rapamune therapy, during Rapamune therapy, and for 12 weeks after Rapamune therapy has been stopped. Rapamune should be used during pregnancy only if the potential benefit outweighs the potential risk to the embryo/fetus.
Use during lactation
Sirolimus is excreted in trace amounts in milk of lactating rats. It is not known whether sirolimus is excreted in human milk. The pharmacokinetic and safety profiles of sirolimus in infants are not known. Because many drugs are excreted in human milk and because of the potential for adverse reactions in nursing infants from sirolimus, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric use
The safety and efficacy of Rapamune ® in pediatric patients below the age of 13 years have not been established.
The safety and efficacy of Rapamune ® Oral Solution and Rapamune ® Tablets have been established in children aged 13 or older judged to be at low to moderate immunologic risk. Use of Rapamune ® Oral Solution and Rapamune ® Tablets in this subpopulation of children aged 13 or older is supported by evidence from adequate and well-controlled trials of Rapamune ® Oral Solution in adults with additional pharmacokinetic data in pediatric renal transplantation recipients (see CLINICAL PHARMACOLOGY , Special Populations , Pediatric ).
Safety and efficacy information from a controlled clinical trial in pediatric and adolescent (< 18 years of age) renal transplant recipients judged to be at high immunologic risk, defined as a history of one or more acute rejection episodes and/or the presence of chronic allograft nephropathy, do not support the chronic use of Rapamune ® Oral Solution or Tablets in combination with calcineurin inhibitors and corticosteroids, due to the increased risk of lipid abnormalities and deterioration of renal function associated with these immunosuppressive regimens, without increased benefit with respect to acute rejection, graft survival, or patient survival (see CLINICAL STUDIES , Pediatrics ).
Geriatric use
Clinical studies of Rapamune Oral Solution or Tablets did not include sufficient numbers of patients aged 65 years and over to determine whether safety and efficacy differ in this population from younger patients. Data pertaining to sirolimus trough concentrations suggest that dose adjustments based upon age in geriatric renal patients are not necessary.
ADVERSE REACTIONS
Rapamune ® Oral Solution: The incidence of adverse reactions was determined in two randomized, double-blind, multicenter controlled trials in which 499 renal transplant patients received Rapamune Oral Solution 2 mg/day, 477 received Rapamune Oral Solution 5 mg/day, 160 received azathioprine, and 124 received placebo. All patients were treated with cyclosporine and corticosteroids. Data (>/= 12 months post-transplant) presented in the table below show the adverse reactions that occurred in any treatment group with an incidence of >/= 20%.
Specific adverse reactions associated with the administration of Rapamune (sirolimus) Oral Solution occurred at a significantly higher frequency than in the respective control group. For both Rapamune Oral Solution 2 mg/day and 5 mg/day these include hypercholesterolemia, hyperlipemia, hypertension, and rash; for Rapamune Oral Solution 2 mg/day acne; and for Rapamune Oral Solution 5 mg/day anemia, arthralgia, diarrhea, hypokalemia, and thrombocytopenia. The elevations of triglycerides and cholesterol and decreases in platelets and hemoglobin occurred in a dose-related manner in patients receiving Rapamune.
Patients maintained on Rapamune Oral Solution 5 mg/day, when compared with patients on Rapamune Oral Solution 2 mg/day, demonstrated an increased incidence of the following adverse events: anemia, leukopenia, thrombocytopenia, hypokalemia, hyperlipemia, fever, and diarrhea.
In general, adverse events related to the administration of Rapamune were dependent on dose/concentration.
ADVERSE EVENTS OCCURRING AT A FREQUENCY OF >/= 20% IN ANY TREATMENT GROUP IN PREVENTION OF ACUTE RENAL REJECTION TRIALS (%) AT >/= 12 MONTHS
POST-TRANSPLANTATION FOR STUDIES 1 AND 2 aBody SystemRapamune ®
Oral Solution
-------2 mg/day-----Rapamune ®
Oral Solution
-------5 mg/day-----Azathioprine
2-3 mg/kg/dayPlacebo Adverse EventStudy 1
(n = 281)Study 2
(n = 218)Study 1
(n = 269)Study 2
(n = 208)Study 1
(n = 160)Study 2
(n = 124)Body As A WholeAbdominal pain28 29 30 36 29 30 Asthenia38 22 40 28 37 28 Back pain16 23 26 22 23 20 Chest pain16 18 19 24 16 19 Fever27 23 33 34 33 35 Headache23 34 27 34 21 31 Pain24 33 29 29 30 25 Cardiovascular SystemHypertension43 45 39 49 29 48 Digestive SystemConstipation28 36 34 38 37 31 Diarrhea32 25 42 35 28 27 Dyspepsia17 23 23 25 24 34 Nausea31 25 36 31 39 29 Vomiting21 19 25 25 31 21 Hemic And Lymphatic SystemAnemia27 23 37 33 29 21 Leukopenia9 9 15 13 20 8 Thrombocytopenia13 14 20 30 9 9 Metabolic And NutritionalCreatinine increased35 39 37 40 28 38 Edema24 20 16 18 23 15 Hypercholesteremia38 43 42 46 33 23 (See WARNINGS and PRECAUTIONS )Hyperkalemia15 17 12 14 24 27 Hyperlipemia38 45 44 57 28 23 (See WARNINGS and PRECAUTIONS )Hypokalemia17 11 21 17 11 9 Hypophosphatemia20 15 23 19 20 19 Peripheral edema60 54 64 58 58 48 Weight gain21 11 15 8 19 15 Musculoskeletal SystemArthralgia25 25 27 31 21 18 Nervous SystemInsomnia14 13 22 14 18 8 Tremor31 21 30 22 28 19 Respiratory SystemDyspnea22 24 28 30 23 30 Pharyngitis17 16 16 21 17 22 Upper respiratory infection20 26 24 23 13 23 Skin And AppendagesAcne31 22 20 22 17 19 Rash12 10 13 20 6 6 Urogenital SystemUrinary tract infection20 26 23 33 31 26 a: Patients received cyclosporine and corticosteroids.
With longer term follow-up, the adverse event profile remained similar. Some new events became significantly different among the treatment groups. For events which occurred at a frequency of >/= 20% by 24 months for Study 1 and 36 months for Study 2, only the incidence of edema became significantly higher in both Rapamune groups as compared with the control group. The incidence of headache became significantly more common in the Rapamune 5mg/day group as compared with control therapy.
At 24 months for Study 1, the following treatment-emergent infections were significantly different among the treatment groups: bronchitis, Herpes simplex, pneumonia, pyelonephritis, and upper respiratory infections. In each instance, the incidence was highest in the Rapamune 5 mg/day group, lower in the Rapamune 2 mg/day group and lowest in the azathioprine group. Except for upper respiratory infections in the Rapamune 5 mg/day cohort, the remainder of events occurred with a frequency of < 20%.
At 36 months in Study 2 only the incidence of treatment-emergent Herpes simplex was significantly different among the treatment groups, being higher in the Rapamune 5 mg/day group than either of the other groups.
The table below summarizes the incidence of malignancies in the two controlled trials for the prevention of acute rejection. At 24 (Study 1) and 36 months (Study 2) there were no significant differences among treatment groups.
INCIDENCE (%) OF MALIGNANCIES IN STUDIES 1 (24 MONTHS) AND STUDY 2
(36 MONTHS) POST-TRANSPLANT a , bRapamune ®
Oral Solution
2 mg/dayRapamune ®
Oral Solution
5 mg/dayAzathioprine
2-3 mg/kg/day
PlaceboMalignancyStudy 1
(n = 284)Study 2
(n = 227)Study 1
(n = 274)Study 2
(n = 219)Study 1
(n = 161)Study 2
(n = 130)Lymphoma/
lymphoproliferative disease0.7 1.8 1.1 3.2 0.6 0.8 Skin CarcinomaAny Squamous Cell c0.4 2.7 2.2 0.9 3.8 3.0 Any Basal Cell c0.7 2.2 1.5 1.8 2.5 5.3 Melanoma0.0 0.4 0.0 1.4 0.0 0.0 Miscellaneous/Not Specified0.0 0.0 0.0 0.0 0.0 0.8 Total1.1 4.4 3.3 4.1 4.3 7.7 Other Malignancy1.1 2.2 1.5 1.4 0.6 2.3 a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.c: Patients may be counted in more than one category.
Among the adverse events that were reported at a rate of >/=3% and <20% at 12 months, the following were more prominent in patients maintained on Rapamune 5 mg/day, when compared with patients on Rapamune 2 mg/day: epistaxis, lymphocele, insomnia, thrombotic thrombocytopenic purpura (hemolytic-uremic syndrome), skin ulcer, increased LDH, hypotension, facial edema.
The following adverse events were reported with >/=3% and <20% incidence in patients in any Rapamune treatment group in the two controlled clinical trials for the prevention of acute rejection, BODY AS A WHOLE: abdomen enlarged, abscess, ascites, cellulitis, chills, face edema, flu syndrome, generalized edema, hernia, Herpes zoster infection, lymphocele, malaise, pelvic pain, peritonitis, sepsis; CARDIOVASCULAR SYSTEM: atrial fibrillation, congestive heart failure, hemorrhage, hypervolemia, hypotension, palpitation, peripheral vascular disorder, postural hypotension, syncope, tachycardia, thrombophlebitis, thrombosis, vasodilatation, venous thromboembolism; DIGESTIVE SYSTEM: anorexia, dysphagia, eructation, esophagitis, flatulence, gastritis, gastroenteritis, gingivitis, gum hyperplasia, ileus, liver function tests abnormal, mouth ulceration, oral moniliasis, stomatitis; ENDOCRINE SYSTEM: Cushing's syndrome, diabetes mellitus, glycosuria; HEMIC AND LYMPHATIC SYSTEM: ecchymosis, leukocytosis, lymphadenopathy, polycythemia, thrombotic thrombocytopenic purpura (hemolytic-uremic syndrome); METABOLIC AND NUTRITIONAL: acidosis, alkaline phosphatase increased, BUN increased, creatine phosphokinase increased, dehydration, healing abnormal, hypercalcemia, hyperglycemia, hyperphosphatemia, hypocalcemia, hypoglycemia, hypomagnesemia, hyponatremia, lactic dehydrogenase increased, AST/SGOT increased, ALT/SGPT increased, weight loss; MUSCULOSKELETAL SYSTEM: arthrosis, bone necrosis, leg cramps, myalgia, osteoporosis, tetany; NERVOUS SYSTEM: anxiety, confusion, depression, dizziness, emotional lability, hypertonia, hypesthesia, hypotonia, insomnia, neuropathy, paresthesia, somnolence; RESPIRATORY SYSTEM: asthma, atelectasis, bronchitis, cough increased, epistaxis, hypoxia, lung edema, pleural effusion, pneumonia, rhinitis, sinusitis; SKIN AND APPENDAGES: fungal dermatitis, hirsutism, pruritus, skin hypertrophy, skin ulcer, sweating; SPECIAL SENSES: abnormal vision, cataract, conjunctivitis, deafness, ear pain, otitis media, tinnitus; UROGENITAL SYSTEM: albuminuria, bladder pain, dysuria, hematuria, hydronephrosis, impotence, kidney pain, kidney tubular necrosis, nocturia, oliguria, pyelonephritis, pyuria, scrotal edema, testis disorder, toxic nephropathy, urinary frequency, urinary incontinence, urinary retention.
Less frequently occurring adverse events included: mycobacterial infections, Epstein-Barr virus infections, and pancreatitis.
Among the events which were reported at an incidence of >/= 3% and < 20% by 24 months for Study 1 and 36 months for Study 2, tachycardia and Cushing's syndrome were reported significantly more commonly in both Rapamune groups as compared with the control therapy. Events that were reported more commonly in the Rapamune 5 mg/day group than either the Rapamune 2 mg/day group and/or control group were: abnormal healing, bone necrosis, chills, congestive heart failure, dysuria, hernia, hirsutism, urinary frequency, and lymphadenopathy.
Rapamune ® Tablets: The safety profile of the tablet did not differ from that of the oral solution formulation. The incidence of adverse reactions up to 12 months was determined in a randomized, multicenter controlled trial (Study 3) in which 229 renal transplant patients received Rapamune Oral Solution 2 mg once daily and 228 patients received Rapamune Tablets 2 mg once daily. All patients were treated with cyclosporine and corticosteroids. The adverse reactions that occurred in either treatment group with an incidence of >/= 20% in Study 3 are similar to those reported for Studies 1 and 2. There was no notable difference in the incidence of these adverse events between treatment groups (oral solution versus tablets) in Study 3, with the exception of acne, which occurred more frequently in the oral solution group, and tremor which occurred more frequently in the tablet group, particularly in Black patients.
The adverse events that occurred in patients with an incidence of >/=3% and <20% in either treatment group in Study 3 were similar to those reported in Studies 1 and 2. There was no notable difference in the incidence of these adverse events between treatment groups (oral solution versus tablets) in Study 3, with the exception of hypertonia, which occurred more frequently in the oral solution group and diabetes mellitus which occurred more frequently in the tablet group. Hispanic patients in the tablet group experienced hyperglycemia more frequently than Hispanic patients in the oral solution group. In Study 3 alone, menorrhagia, metrorrhagia, and polyuria occurred with an incidence of >/=3% and <20%.
The clinically important opportunistic or common transplant-related infections were identical in all three studies and the incidences of these infections were similar in Study 3 compared with Studies 1 and 2. The incidence rates of these infections were not significantly different between the oral solution and tablet treatment groups in Study 3.
In Study 3 (at 12 months), there were two cases of lymphoma/lymphoproliferative disorder in the oral solution treatment group (0.8%) and two reported cases of lymphoma/lymphoproliferative disorder in the tablet treatment group (0.8%). These differences were not statistically significant and were similar to the incidences observed in Studies 1 and 2.
Rapamune following cyclosporine withdrawal: The incidence of adverse reactions was determined through 36 months in a randomized, multicenter controlled trial (Study 4) in which 215 renal transplant patients received Rapamune as a maintenance regimen following cyclosporine withdrawal and 215 patients received Rapamune with cyclosporine therapy. All patients were treated with corticosteroids. The safety profile prior to randomization (start of cyclosporine withdrawal) was similar to that of the 2-mg Rapamune groups in Studies 1, 2, and 3. Following randomization (at 3 months) patients who had cyclosporine eliminated from their therapy experienced significantly higher incidences of abnormal liver function tests (including increased AST/SGOT and increased ALT/SGPT), hypokalemia, thrombocytopenia, abnormal healing, ileus, and rectal disorder. Conversely, the incidence of hypertension, cyclosporine toxicity, increased creatinine, abnormal kidney function, toxic nephropathy, edema, hyperkalemia, hyperuricemia, and gum hyperplasia was significantly higher in patients who remained on cyclosporine than those who had cyclosporine withdrawn from therapy. Mean systolic and diastolic blood pressure improved significantly following cyclosporine withdrawal.
In Study 4, at 36 months, the incidence of Herpes zoster infection was significantly lower in patients receiving Rapamune following cyclosporine withdrawal compared with patients who continued to receive Rapamune and cyclosporine.
The incidence of malignancies in Study 4 is presented in the table below. In Study 4, the incidence of lymphoma/lymphoproliferative disease was similar in all treatment groups. The overall incidence of malignancy was higher in patients receiving Rapamune plus cyclosporine compared with patients who had cyclosporine withdrawn.
INCIDENCE (%) OF MALIGNANCIES IN STUDY 4 AT 36 MONTHS POST-TRANSPLANT a , b MalignancyNonrandomized
(n = 95)Rapamune with
Cyclosporine
Therapy
(n = 215)Rapamune
Following
Cyclosporine
Withdrawal
(n = 215)Lymphoma/lymphoproliferative disease1.1 1.4 0.5 Skin CarcinomaAny Squamous Cell c1.1 1.9 2.3 Any Basal Cell c3.2 4.7 2.3 Melanoma0.0 0.5 0.0 Miscellaneous/Not Specified1.1 0.9 0.0 Total4.2 6.5 3.7 Other Malignancy1.1 3.3 1.4 a: Patients received cyclosporine and corticosteroids.b: Includes patients who prematurely discontinued treatment.c: Patients may be counted in more than one category.Pediatrics: Safety was assessed in the controlled clinical trial in pediatric (< 18 years of age) renal transplant patients considered high immunologic risk, defined as a history of one or more acute allograft rejection episodes and/or the presence of chronic allograft nephropathy on a renal biopsy (see CLINICAL STUDIES ). The use of Rapamune ® in combination with calcineurin inhibitors and corticosteroids was associated with an increased risk of deterioration of renal function, serum lipid abnormalities (including but not limited to increased serum triglycerides and cholesterol), and urinary tract infections.
Other clinical experience: Cases of interstitial lung disease (including pneumonitis, and infrequently bronchiolitis obliterans organizing pneumonia [BOOP] and pulmonary fibrosis), some fatal, with no identified infectious etiology have occurred in patients receiving immunosuppressive regimens including Rapamune. In some cases, the interstitial lung disease has resolved upon discontinuation or dose reduction of Rapamune. The risk may be increased as the sirolimus trough concentration increases (see PRECAUTIONS , General , Interstitial Lung Disease ). There have been reports of neutropenia and rare reports of pancytopenia. Hypersensitivity reactions, including anaphylactic/anaphylactoid reactions, have been associated with the administration of sirolimus (see WARNINGS ). Hepatotoxicity has been reported, including fatal hepatic necrosis with elevated sirolimus trough concentrations. There have been rare reports of lymphedema. Abnormal healing following transplant surgery has been reported, including fascial dehiscence and anastomotic disruption (e.g., wound, vascular, airway, ureteral, biliary).
The safety and efficacy of conversion from calcineurin inhibitors to sirolimus in maintenance renal transplant population has not been established. In an ongoing study evaluating the safety and efficacy of conversion from calcineurin inhibitors to sirolimus (target concentrations of 12-20 ng/mL) in maintenance renal transplant patients; enrollment was stopped in the subset of patients (n=90) with a baseline glomerular filtration rate of less than 40 mL/min. There was a higher rate of serious adverse events including pneumonia, acute rejection, graft loss and death in this sirolimus treatment arm.
OVERDOSAGE
Reports of overdose with Rapamune have been received; however, experience has been limited. In general, the adverse effects of overdose are consistent with those listed in the ADVERSE REACTIONS section (see ADVERSE REACTIONS ).
General supportive measures should be followed in all cases of overdose. Based on the poor aqueous solubility and high erythrocyte and plasma protein binding of sirolimus, it is anticipated that sirolimus is not dialyzable to any significant extent. In mice and rats, the acute oral lethal dose was greater than 800 mg/kg.
DOSAGE AND ADMINISTRATION
It is recommended that Rapamune Oral Solution and Tablets be used initially in a regimen with cyclosporine and corticosteroids. Cyclosporine withdrawal is recommended 2 to 4 months after transplantation in patients at low to moderate immunologic risk.
The safety and efficacy of cyclosporine withdrawal in high-risk patients have not been adequately studied and it is therefore not recommended. This includes patients with Banff grade III acute rejection or vascular rejection prior to cyclosporine withdrawal, those who are dialysis-dependent, or with serum creatinine > 4.5 mg/dL, black patients, re-transplants, multi-organ transplants, patients with high panel of reactive antibodies (See INDICATIONS AND USAGE and CLINICAL STUDIES ).
Two-mg of Rapamune oral solution has been demonstrated to be clinically equivalent to 2-mg Rapamune oral tablets and hence, are interchangeable on a mg to mg basis. However, it is not known if higher doses of Rapamune oral solution are clinically equivalent to higher doses of tablets on a mg to mg basis. (See CLINICAL PHARMACOLOGY : Absorption ). Rapamune is to be administered orally once daily.
Rapamune and cyclosporine combination therapy: The initial dose of Rapamune should be administered as soon as possible after transplantation. For de novo transplant recipients, a loading dose of Rapamune of 3 times the maintenance dose should be given. A daily maintenance dose of 2-mg is recommended for use in renal transplant patients, with a loading dose of 6 mg. Although a daily maintenance dose of 5 mg, with a loading dose of 15 mg was used in clinical trials of the oral solution and was shown to be safe and effective, no efficacy advantage over the 2-mg dose could be established for renal transplant patients. Patients receiving 2 mg of Rapamune Oral Solution per day demonstrated an overall better safety profile than did patients receiving 5 mg of Rapamune Oral Solution per day.
Rapamune following cyclosporine withdrawal: Initially, patients considered for cyclosporine withdrawal should be receiving Rapamune and cyclosporine combination therapy. At 2 to 4 months following transplantation, cyclosporine should be progressively discontinued over 4 to 8 weeks and the Rapamune ® dose should be adjusted to obtain whole blood trough concentrations within the range of 12 to 24 ng/mL (chromatographic method). Therapeutic drug monitoring should not be the sole basis for adjusting Rapamune therapy. Careful attention should be made to clinical signs/symptoms, tissue biopsy, and laboratory parameters. Cyclosporine inhibits the metabolism and transport of sirolimus, and consequently, sirolimus concentrations will decrease when cyclosporine is discontinued unless the Rapamune dose is increased. The Rapamune ® dose will need to be approximately 4-fold higher to account for both the absence of the pharmacokinetic interaction (approximately 2-fold increase) and the augmented immunosuppressive requirement in the absence of cyclosporine (approximately 2-fold increase).
Frequent Rapamune ® dose adjustments based on non-steady-state sirolimus concentrations can lead to overdosing or underdosing because sirolimus has a long half-life. Once Rapamune ® maintenance dose is adjusted, patients should be retained on the new maintenance dose at least for 7 to 14 days before further dosage adjustment with concentration monitoring. In most patients dose adjustments can be based on simple proportion: new Rapamune ® dose = current dose x (target concentration/current concentration). A loading dose should be considered in addition to a new maintenance dose when it is necessary to considerably increase sirolimus trough concentrations: Rapamune ® loading dose = 3 × (new maintenance dose - current maintenance dose). The maximum Rapamune ® dose administered on any day should not exceed 40 mg. If an estimated daily dose exceeds 40 mg due to the addition of a loading dose, the loading dose should be administered over 2 days. Sirolimus trough concentrations should be monitored at least 3 to 4 days after a loading dose(s).
To minimize the variability of exposure to Rapamune, this drug should be taken consistently with or without food. Grapefruit juice reduces CYP3A4-mediated drug metabolism and potentially enhances P-gp mediated drug counter-transport from enterocytes of the small intestine. This juice must not be administered with Rapamune or used for dilution.
It is recommended that sirolimus be taken 4 hours after administration of cyclosporine oral solution (MODIFIED) and/or cyclosporine capsules (MODIFIED).
Dosage Adjustments
The initial dosage in patients >/=13 years who weigh less than 40 kg should be adjusted, based on body surface area, to 1 mg/m 2 /day. The loading dose should be 3 mg/m 2 .
Patients with Hepatic Impairment:
It is recommended that the maintenance dose of Rapamune be reduced by approximately one third in patients with hepatic impairment.
Patients with Renal Impairment:
It is not necessary to modify the Rapamune loading dose. Dosage need not be adjusted because of impaired renal function.
Blood Concentration Monitoring
Whole blood trough concentrations of sirolimus should be monitored in patients receiving concentration-controlled Rapamune ® . Monitoring is also necessary in pediatric patients, in patients with hepatic impairment, during concurrent administration of CYP3A4 and/or P-gp inducers and inhibitors, and/or if cyclosporine dosage is markedly changed or discontinued (see DOSAGE AND ADMINISTRATION ).
In controlled clinical trials with concomitant cyclosporine (Studies 1 and 2), mean sirolimus whole blood trough concentrations through month 12 following transplantation, as measured by immunoassay, were 9 ng/mL (range 4.5-14 ng/mL [10 th to 90 th percentile]) for the 2 mg/day treatment group, and 17 ng/mL (range 10-28 ng/mL [10 th to 90 th percentile]) for the 5 mg/day dose.
In a controlled clinical trial with cyclosporine withdrawal (Study 4), the mean sirolimus whole blood trough concentrations during months 4 through 12 following transplantation, as measured by immunoassay, were 10.7 ng/mL (range 6.3-16.0 ng/mL [10 th to 90 th percentile]) in the concomitant Rapamune and cyclosporine treatment group (n = 205) and were 23.3 ng/mL (range 17.0-29.0 ng/mL [10 th to 90 th percentile]) in the cyclosporine withdrawal treatment group (n = 200).
Results from other assays may differ from those with an immunoassay. On average, chromatographic methods (HPLC UV or LC/MS/MS) yield results that are approximately 20% lower than the immunoassay for whole blood concentration determinations. Adjustments to the targeted range should be made according to the assay utilized to determine sirolimus trough concentrations. Therefore, comparison between concentrations in the published literature and an individual patient concentration using current assays must be made with detailed knowledge of the assay methods employed. A discussion of the different assay methods is contained in Clinical Therapeutics , Volume 22, Supplement B, April 2000.
Instructions for Dilution and Administration of Rapamune ® Oral Solution Bottles
The amber oral dose syringe should be used to withdraw the prescribed amount of Rapamune ® Oral Solution from the bottle. Empty the correct amount of Rapamune from the syringe into only a glass or plastic container holding at least two (2) ounces (1/4 cup, 60 mL) of water or orange juice. No other liquids, including grapefruit juice, should be used for dilution. Stir vigorously and drink at once. Refill the container with an additional volume (minimum of four [4] ounces [1/2 cup, 120 mL]) of water or orange juice, stir vigorously, and drink at once.
Rapamune Oral Solution contains polysorbate-80, which is known to increase the rate of di-(2-ethylhexyl)phthalate (DEHP) extraction from polyvinyl chloride (PVC). This should be considered during the preparation and administration of Rapamune Oral Solution. It is important that the recommendations in DOSAGE AND ADMINISTRATION be followed closely.
Handling and Disposal
Since Rapamune is not absorbed through the skin, there are no special precautions. However, if direct contact with the skin or mucous membranes occurs, wash thoroughly with soap and water; rinse eyes with plain water.
HOW SUPPLIED
Rapamune ® Oral Solution is supplied at a concentration of 1 mg/mL in:
Cartons:
NDC # 0008-1030-06 containing a 2 oz (60 mL fill) amber glass bottle.
In addition to the bottles, each carton is supplied with an oral syringe adapter for fitting into the neck of the bottle, sufficient disposable amber oral syringes and caps for daily dosing, and a carrying case.
Rapamune ® Tablets are available as follows:
1 mg, white, triangular-shaped tablets marked "RAPAMUNE 1 mg" on one side.
NDC # 0008-1031-05, bottle of 100 tablets.
NDC # 0008-1031-10, Redipak ® cartons of 100 tablets (10 blister cards of 10 tablets each).
2 mg, yellow to beige triangular-shaped tablets marked "RAPAMUNE 2 mg" on one side.
NDC # 0008-1032-05, bottle of 100 tablets.
NDC # 0008-1032-10, Redipak ® cartons of 100 tablets (10 blister cards of 10 tablets each [2 x 5]).
Storage
Rapamune ® Oral Solution bottles should be stored protected from light and refrigerated at 2°C to 8°C (36°F to 46°F). Once the bottle is opened, the contents should be used within one month. If necessary, the patient may store the bottles at room temperatures up to 25°C (77°F) for a short period of time (e.g., not more than 15 days for the bottles).
An amber syringe and cap are provided for dosing and the product may be kept in the syringe for a maximum of 24 hours at room temperatures up to 25°C (77°F) or refrigerated at 2°C to 8°C (36°F to 46°F). The syringe should be discarded after one use. After dilution, the preparation should be used immediately.
Rapamune Oral Solution provided in bottles may develop a slight haze when refrigerated. If such a haze occurs allow the product to stand at room temperature and shake gently until the haze disappears. The presence of this haze does not affect the quality of the product.
Rapamune ® Tablets should be stored at 20° to 25°C (USP Controlled Room Temperature) (68° to 77°F). Use cartons to protect blister cards and strips from light. Dispense in a tight, light-resistant container as defined in the USP.
US Pat. Nos.: 5,100,899; 5,212,155; 5,308,847; 5,403,833; 5,536,729.
PATIENT INSTRUCTIONS FOR RAPAMUNE® (SIROLIMUS) ORAL SOLUTION
Bottles
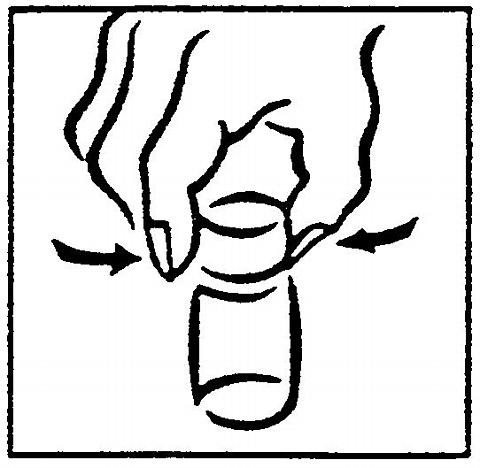
1.Open the solution bottle. Remove the safety cap by squeezing the tabs on the cap and twisting counterclockwise.
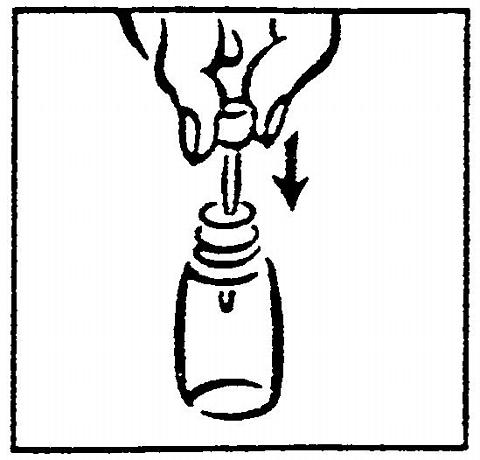
2.On first use, insert the adapter assembly (plastic tube with stopper) tightly into the bottle until it is even with the top of the bottle. Do not remove the adapter assembly from the bottle once inserted.
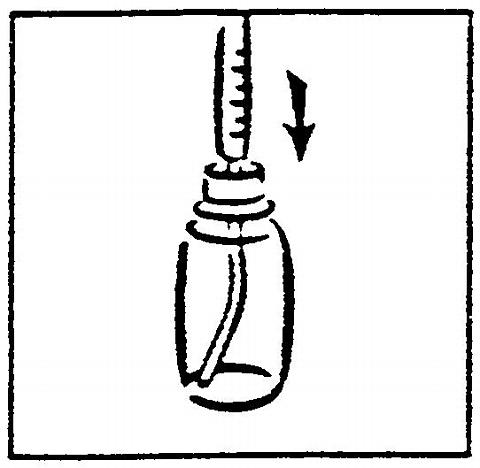
3.For each use, tightly insert one of the amber syringes with the plunger fully depressed into the opening in the adapter.
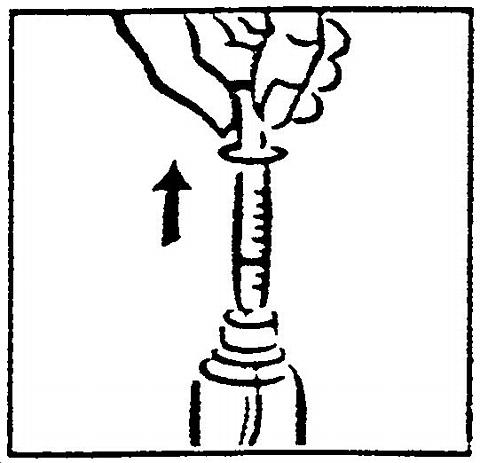
4.Withdraw the prescribed amount of Rapamune ® Oral Solution by gently pulling out the plunger of the syringe until the bottom of the black line of the plunger is even with the appropriate mark on the syringe. Always keep the bottle in an upright position. If bubbles form in the syringe, empty the syringe into the bottle and repeat the procedure.
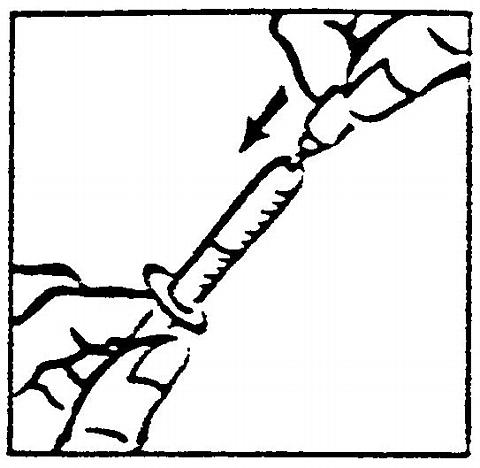
5.You may have been instructed to carry your medication with you. If it is necessary to carry the filled syringe, place a cap securely on the syringe - the cap should snap into place.
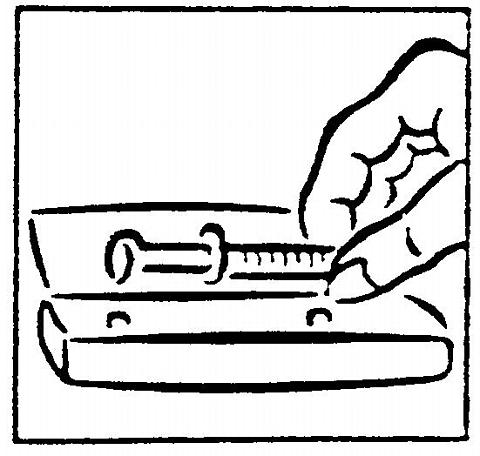
6.Then place the capped syringe in the enclosed carrying case. Once in the syringe, the medication may be kept at room temperature or refrigerated and should be used within 24 hours. Extreme temperatures (below 36°F and above 86°F) should be avoided. Remember to keep this medication out of the reach of children.
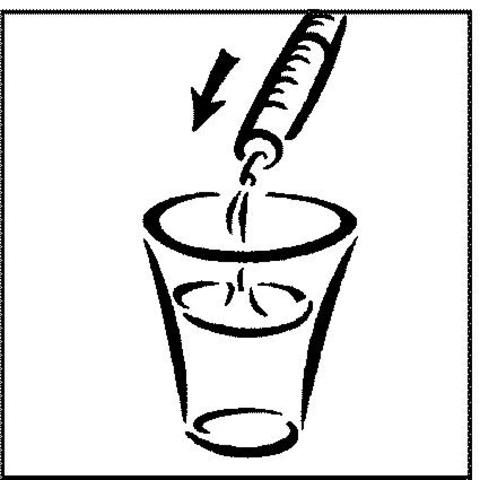
7.Empty the syringe into a glass or plastic cup containing at least 2 ounces (1/4 cup, 60 mL) of water or orange juice, stir vigorously for one (1) minute and drink immediately. Refill the container with at least 4 ounces (1/2 cup, 120 mL) of water or orange juice, stir vigorously again and drink the rinse solution. Apple juice, grapefruit juice, or other liquids are NOT to be used. Only glass or plastic cups should be used to dilute Rapamune ® Oral Solution. The syringe and cap should be used once and then discarded.

8.Always store the bottles of medication in the refrigerator. When refrigerated, a slight haze may develop in the solution. The presence of a haze does not affect the quality of the product. If this happens, bring the Rapamune ® Oral Solution to room temperature and shake until the haze disappears. If it is necessary to wipe clean the mouth of the bottle before returning the product to the refrigerator, wipe with a dry cloth to avoid introducing water, or any other liquid, into the bottle.
Wyeth ®
Wyeth Pharmaceuticals Inc. W10431C010
Philadelphia, PA 19101ET01
Rev 03/05
Subscribe to the "News" RSS Feed 
TOP ۞