-
Trusopt Sterile Ophthalmic Solution (Merck)
DESCRIPTION
TRUSOPT* (dorzolamide hydrochloride ophthalmic solution) is a carbonic anhydrase inhibitor formulated for topical ophthalmic use.
Dorzolamide hydrochloride is described chemically as: (4 S-trans )-4-(ethylamino)-5,6-dihydro-6-methyl-4 H -thieno [2,3- b ]thiopyran-2-sulfonamide 7,7-dioxide monohydrochloride. Dorzolamide hydrochloride is optically active. The specific rotation is
25°
(alpha) (C =1, water) = ~ -17°. 405 Its empirical formula is C 10 H 16 N 2 O 4 S 3 ·HCl and its structural formula is:
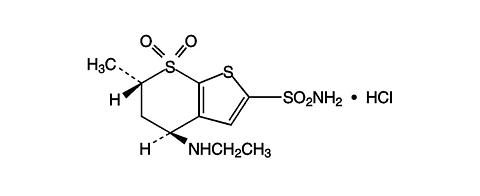
Dorzolamide hydrochloride has a molecular weight of 360.9 and a melting point of about 264°C. It is a white to off-white, crystalline powder, which is soluble in water and slightly soluble in methanol and ethanol.
TRUSOPT Sterile Ophthalmic Solution is supplied as a sterile, isotonic, buffered, slightly viscous, aqueous solution of dorzolamide hydrochloride. The pH of the solution is approximately 5.6, and the osmolarity is 260-330 mOsM. Each mL of TRUSOPT 2% contains 20 mg dorzolamide (22.3 mg of dorzolamide hydrochloride). Inactive ingredients are hydroxyethyl cellulose, mannitol, sodium citrate dihydrate, sodium hydroxide (to adjust pH) and water for injection. Benzalkonium chloride 0.0075% is added as a preservative.
*Registered trademark of Merck & CO., Inc.CLINICAL PHARMACOLOGY
Mechanism of Action
Carbonic anhydrase (CA) is an enzyme found in many tissues of the body including the eye. It catalyzes the reversible reaction involving the hydration of carbon dioxide and the dehydration of carbonic acid. In humans, carbonic anhydrase exists as a number of isoenzymes, the most active being carbonic anhydrase II (CA-II), found primarily in red blood cells (RBCs), but also in other tissues. Inhibition of carbonic anhydrase in the ciliary processes of the eye decreases aqueous humor secretion, presumably by slowing the formation of bicarbonate ions with subsequent reduction in sodium and fluid transport. The result is a reduction in intraocular pressure (IOP).
TRUSOPT Ophthalmic Solution contains dorzolamide hydrochloride, an inhibitor of human carbonic anhydrase II. Following topical ocular administration, TRUSOPT reduces elevated intraocular pressure. Elevated intraocular pressure is a major risk factor in the pathogenesis of optic nerve damage and glaucomatous visual field loss.
Pharmacokinetics/Pharmacodynamics
When topically applied, dorzolamide reaches the systemic circulation. To assess the potential for systemic carbonic anhydrase inhibition following topical administration, drug and metabolite concentrations in RBCs and plasma and carbonic anhydrase inhibition in RBCs were measured. Dorzolamide accumulates in RBCs during chronic dosing as a result of binding to CA-II. The parent drug forms a single N-desethyl metabolite, which inhibits CA-II less potently than the parent drug but also inhibits CA-I. The metabolite also accumulates in RBCs where it binds primarily to CA-I. Plasma concentrations of dorzolamide and metabolite are generally below the assay limit of quantitation (15nM). Dorzolamide binds moderately to plasma proteins (approximately 33%). Dorzolamide is primarily excreted unchanged in the urine; the metabolite also is excreted in urine. After dosing is stopped, dorzolamide washes out of RBCs nonlinearly, resulting in a rapid decline of drug concentration initially, followed by a slower elimination phase with a half-life of about four months.
To simulate the systemic exposure after long-term topical ocular administration, dorzolamide was given orally to eight healthy subjects for up to 20 weeks. The oral dose of 2 mg b.i.d. closely approximates the amount of drug delivered by topical ocular administration of TRUSOPT 2% t.i.d. Steady state was reached within 8 weeks. The inhibition of CA-II and total carbonic anhydrase activities was below the degree of inhibition anticipated to be necessary for a pharmacological effect on renal function and respiration in healthy individuals.
Clinical Studies
The efficacy of TRUSOPT was demonstrated in clinical studies in the treatment of elevated intraocular pressure in patients with glaucoma or ocular hypertension (baseline IOP >/=23 mmHg). The IOP-lowering effect of TRUSOPT was approximately 3 to 5 mmHg throughout the day and this was consistent in clinical studies of up to one year duration.
The efficacy of TRUSOPT when dosed less frequently than three times a day (alone or in combination with other products) has not been established.
In a one year clinical study, the effect of TRUSOPT 2% t.i.d. on the corneal endothelium was compared to that of betaxolol ophthalmic solution b.i.d. and timolol maleate ophthalmic solution 0.5% b.i.d. There were no statistically significant differences between groups in corneal endothelial cell counts or in corneal thickness measurements. There was a mean loss of approximately 4% in the endothelial cell counts for each group over the one year period.
INDICATIONS AND USAGE
TRUSOPT Ophthalmic Solution is indicated in the treatment of elevated intraocular pressure in patients with ocular hypertension or open-angle glaucoma.
CONTRAINDICATIONS
TRUSOPT is contraindicated in patients who are hypersensitive to any component of this product.
WARNINGS
TRUSOPT is a sulfonamide and although administered topically is absorbed systemically. Therefore, the same types of adverse reactions that are attributable to sulfonamides may occur with topical administration with TRUSOPT. Fatalities have occurred, although rarely, due to severe reactions to sulfonamides including Stevens-Johnson syndrome, toxic epidermal necrolysis, fulminant hepatic necrosis, agranulocytosis, aplastic anemia, and other blood dyscrasias. Sensitization may recur when a sulfonamide is readministered irrespective of the route of administration. If signs of serious reactions or hypersensitivity occur, discontinue the use of this preparation.
PRECAUTIONS
General
The management of patients with acute angle-closure glaucoma requires therapeutic interventions in addition to ocular hypotensive agents. TRUSOPT has not been studied in patients with acute angle-closure glaucoma.
TRUSOPT has not been studied in patients with severe renal impairment (CrCl < 30 mL/min). Because TRUSOPT and its metabolite are excreted predominantly by the kidney, TRUSOPT is not recommended in such patients.
TRUSOPT has not been studied in patients with hepatic impairment and should therefore be used with caution in such patients.
In clinical studies, local ocular adverse effects, primarily conjunctivitis and lid reactions, were reported with chronic administration of TRUSOPT. Many of these reactions had the clinical appearance and course of an allergic-type reaction that resolved upon discontinuation of drug therapy. If such reactions are observed, TRUSOPT should be discontinued and the patient evaluated before considering restarting the drug. (See ADVERSE REACTIONS .)
There is a potential for an additive effect on the known systemic effects of carbonic anhydrase inhibition in patients receiving an oral carbonic anhydrase inhibitor and TRUSOPT. The concomitant administration of TRUSOPT and oral carbonic anhydrase inhibitors is not recommended.
There have been reports of bacterial keratitis associated with the use of multiple-dose containers of topical ophthalmic products. These containers had been inadvertently contaminated by patients who, in most cases, had a concurrent corneal disease or a disruption of the ocular epithelial surface.
Choroidal detachment has been reported with administration of aqueous suppressant therapy (e.g., dorzolamide) after filtration procedures.
Information for Patients
TRUSOPT is a sulfonamide and although administered topically is absorbed systemically. Therefore the same types of adverse reactions that are attributable to sulfonamides may occur with topical administration. Patients should be advised that if serious or unusual reactions or signs of hypersensitivity occur, they should discontinue the use of the product (see WARNINGS ).
Patients should be advised that if they develop any ocular reactions, particularly conjunctivitis and lid reactions, they should discontinue use and seek their physician's advice.
Patients should be instructed to avoid allowing the tip of the dispensing container to contact the eye or surrounding structures.
Patients should also be instructed that ocular solutions, if handled improperly or if the tip of the dispensing container contacts the eye or surrounding structures, can become contaminated by common bacteria known to cause ocular infections. Serious damage to the eye and subsequent loss of vision may result from using contaminated solutions.
Patients also should be advised that if they have ocular surgery or develop an intercurrent ocular condition (e.g., trauma or infection), they should immediately seek their physician's advice concerning the continued use of the present multidose container.
If more than one topical ophthalmic drug is being used, the drugs should be administered at least ten minutes apart.
Patients should be advised that TRUSOPT contains benzalkonium chloride which may be absorbed by soft contact lenses. Contact lenses should be removed prior to administration of the solution. Lenses may be reinserted 15 minutes following TRUSOPT administration.
Drug Interactions
Although acid-base and electrolyte disturbances were not reported in the clinical trials with TRUSOPT, these disturbances have been reported with oral carbonic anhydrase inhibitors and have, in some instances, resulted in drug interactions (e.g., toxicity associated with high-dose salicylate therapy). Therefore, the potential for such drug interactions should be considered in patients receiving TRUSOPT.
Carcinogenesis, Mutagenesis, Impairment of Fertility
In a two-year study of dorzolamide hydrochloride administered orally to male and female Sprague-Dawley rats, urinary bladder papillomas were seen in male rats in the highest dosage group of 20 mg/kg/day (250 times the recommended human ophthalmic dose). Papillomas were not seen in rats given oral doses equivalent to approximately 12 times the recommended human ophthalmic dose. No treatment-related tumors were seen in a 21-month study in female and male mice given oral doses up to 75 mg/kg/day (~900 times the recommended human ophthalmic dose).
The increased incidence of urinary bladder papillomas seen in the high-dose male rats is a class-effect of carbonic anhydrase inhibitors in rats. Rats are particularly prone to developing papillomas in response to foreign bodies, compounds causing crystalluria, and diverse sodium salts.
No changes in bladder urothelium were seen in dogs given oral dorzolamide hydrochloride for one year at 2 mg/kg/day (25 times the recommended human ophthalmic dose) or monkeys dosed topically to the eye at 0.4 mg/kg/day (~5 times the recommended human ophthalmic dose) for one year.
The following tests for mutagenic potential were negative: (1) in vivo (mouse) cytogenetic assay; (2) in vitro chromosomal aberration assay; (3) alkaline elution assay; (4) V-79 assay; and (5) Ames test.
In reproduction studies of dorzolamide hydrochloride in rats, there were no adverse effects on the reproductive capacity of males or females at doses up to 188 or 94 times, respectively, the recommended human ophthalmic dose.
Pregnancy
Teratogenic Effects. Pregnancy Category C. Developmental toxicity studies with dorzolamide hydrochloride in rabbits at oral doses of >/=2.5 mg/kg/day (31 times the recommended human ophthalmic dose) revealed malformations of the vertebral bodies. These malformations occurred at doses that caused metabolic acidosis with decreased body weight gain in dams and decreased fetal weights. No treatment-related malformations were seen at 1.0 mg/kg/day (13 times the recommended human ophthalmic dose). There are no adequate and well-controlled studies in pregnant women. TRUSOPT should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
In a study of dorzolamide hydrochloride in lactating rats, decreases in body weight gain of 5 to 7% in offspring at an oral dose of 7.5 mg/kg/day (94 times the recommended human ophthalmic dose) were seen during lactation. A slight delay in postnatal development (incisor eruption, vaginal canalization and eye openings), secondary to lower fetal body weight, was noted.
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from TRUSOPT, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
Safety and IOP-lowering effects of TRUSOPT have been demonstrated in pediatric patients in a 3-month, multicenter, double-masked, active-treatment-controlled trial.
Geriatric Use
No overall differences in safety and effectiveness have been observed between elderly and younger patients.
ADVERSE REACTIONS
Controlled clinical trials: The most frequent adverse events associated with TRUSOPT were ocular burning, stinging, or discomfort immediately following ocular administration (approximately one-third of patients). Approximately one-quarter of patients noted a bitter taste following administration. Superficial punctate keratitis occurred in 10-15% of patients and signs and symptoms of ocular allergic reaction in approximately 10%. Events occurring in approximately 1-5% of patients were conjunctivitis and lid reactions (see PRECAUTIONS , General ), blurred vision, eye redness, tearing, dryness, and photophobia. Other ocular events and systemic events were reported infrequently, including headache, nausea, asthenia/fatigue; and, rarely, skin rashes, urolithiasis, and iridocyclitis.
In a 3-month, double-masked, active-treatment-controlled, multicenter study in pediatric patients, the adverse experience profile of TRUSOPT was comparable to that seen in adult patients.
Clinical practice: The following adverse events have occurred either at low incidence (<1%) during clinical trials or have been reported during the use of TRUSOPT in clinical practice where these events were reported voluntarily from a population of unknown size and frequency of occurrence cannot be determined precisely. They have been chosen for inclusion based on factors such as seriousness, frequency of reporting, possible causal connection to TRUSOPT, or a combination of these factors: signs and symptoms of systemic allergic reactions including angioedema, bronchospasm, pruritus, and urticaria; dizziness, paresthesia; ocular pain, transient myopia, choroidal detachment following filtration surgery, eyelid crusting; dyspnea; contact dermatitis, epistaxis, dry mouth and throat irritation.
OVERDOSAGE
Electrolyte imbalance, development of an acidotic state, and possible central nervous system effects may occur. Serum electrolyte levels (particularly potassium) and blood pH levels should be monitored.
DOSAGE AND ADMINISTRATION
The dose is one drop of TRUSOPT Ophthalmic Solution in the affected eyes(s) three times daily.
TRUSOPT may be used concomitantly with other topical ophthalmic drug products to lower intraocular pressure. If more than one topical ophthalmic drug is being used, the drugs should be administered at least ten minutes apart.
HOW SUPPLIED
TRUSOPT Ophthalmic Solution is a slightly opalescent, nearly colorless, slightly viscous solution.
No. 3519--TRUSOPT Ophthalmic Solution 2% is supplied in an OCUMETER®* PLUS container, a white, translucent, HDPE plastic ophthalmic dispenser with a controlled drop tip and a white polystyrene cap with orange label as follows:
NDC 0006-3519-35, 5 mL, in a 7.5 mL capacity bottle
NDC 0006-3519-36, 10 mL, in an 18 mL capacity bottle.
Storage
Store TRUSOPT Ophthalmic Solution at 15-30°C (59-86°F). Protect from light.
Rx only
INSTRUCTIONS FOR USE
Please follow these instructions carefully when using TRUSOPT*. Use TRUSOPT as prescribed by your doctor.
- If you use other topically applied ophthalmic medications, they should be administered at least 10 minutes before or after TRUSOPT.
- Wash hands before each use.
-
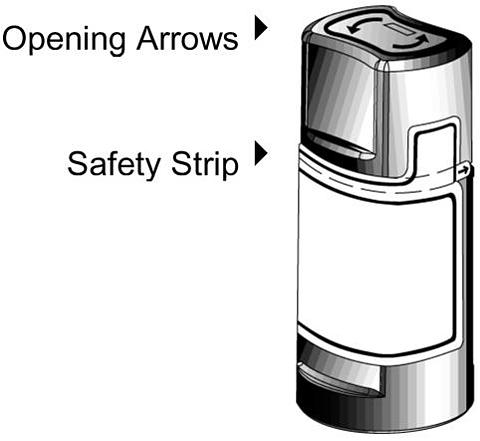
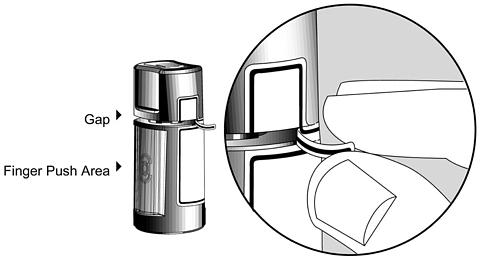
Before using the medication for the first time, be sure the Safety Strip on the front of the bottle is unbroken. A gap between the bottle and the cap is normal for an unopened bottle.
-
Tear off the Safety Strip to break the seal.
-
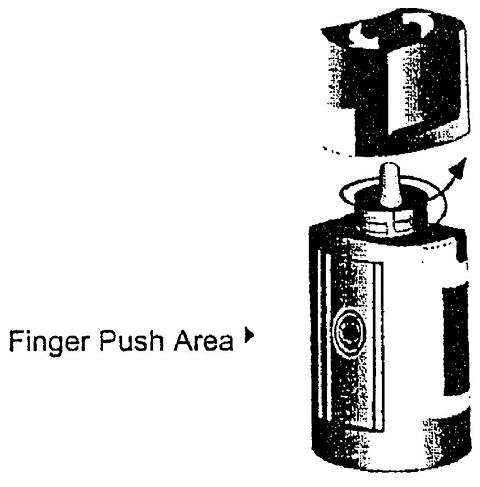
To open the bottle, unscrew the cap by turning as indicated by the arrows on the top of the cap. When opening the bottle for the first time, do not pull the cap directly up and away from the bottle. Pulling the cap directly up will prevent your dispenser from operating properly.
-
Tilt your head back and pull your lower eyelid down slightly to form a pocket between your eyelid and your eye.
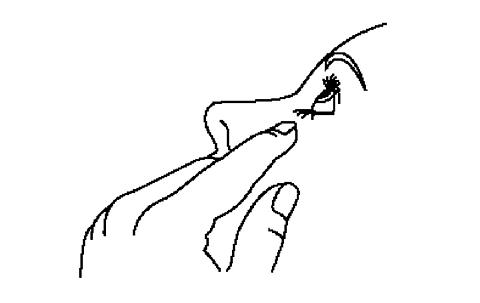
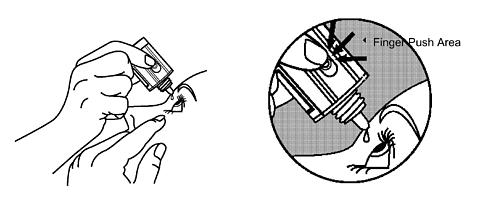
-
Invert the bottle, and press lightly with the thumb or index finger over the "Finger Push Area" (as shown) until a single drop is dispensed into the eye as directed by your doctor. If drop dispensing is difficult after opening for the first time, replace the cap on the bottle and tighten (DO NOT OVERTIGHTEN) and then remove by turning the cap in the opposite direction (as indicated by the arrows on the top of the cap).
DO NOT TOUCH YOUR EYE OR EYELID WITH THE DROPPER TIP.
OPHTHALMIC MEDICATIONS, IF HANDLED IMPROPERLY, CAN BECOME CONTAMINATED BY COMMON BACTERIA KNOWN TO CAUSE EYE INFECTIONS. SERIOUS DAMAGE TO THE EYE AND SUBSEQUENT LOSS OF VISION MAY RESULT FROM USING CONTAMINATED OPHTHALMIC MEDICATIONS. IF YOU THINK YOUR MEDICATION MAY BE CONTAMINATED, OR IF YOU DEVELOP AN EYE INFECTION, CONTACT YOUR DOCTOR IMMEDIATELY CONCERNING CONTINUED USE OF THIS BOTTLE. - Repeat steps 6 & 7 with the other eye if instructed to do so by your doctor.
- Replace the cap by turning until it is firmly touching the bottle. The arrow on the left side of the cap must be aligned with the arrow on the left side of the bottle label for proper closure. Attempting to tighten the bottle beyond the resistance point (point at which the arrows on the bottle label and cap are aligned) may damage the bottle and/or cap.
- The dispenser tip is designed to provide a pre-measured drop; therefore, do NOT enlarge the hole of the dispenser tip.
- After you have used all doses, there will be some TRUSOPT left in the bottle. You should not be concerned since an extra amount of TRUSOPT has been added and you will get the full amount of TRUSOPT that your doctor prescribed. Do not attempt to remove excess medicine from the bottle.
WARNING: Keep out of reach of children.
If you have any questions about the use of TRUSOPT, please consult your doctor.
*Registered trademark of Merck & CO., Inc.
Manuf. for:
Merck & Co., Inc., Whitehouse Station, NJ 08889, USA
By: Laboratories Merck Sharp & Dohme-Chibret
63963 Clermont-Ferrand Cedex 9, France
9368206 Issued April 2005
COPYRIGHT© Merck & CO., Inc., 2000
All rights reserved
Subscribe to the "News" RSS Feed 
TOP ۞