-
Zoladex 3-month (Astrazeneca)
DESCRIPTION
ZOLADEX® (goserelin acetate implant), contains a potent synthetic decapeptide analogue of luteinizing hormone-releasing hormone (LHRH), also known as a gonadotropin releasing hormone (GnRH) agonist analogue. Goserelin acetate is chemically described as an acetate salt of [D-Ser(Bu t ) 6 ,Azgly 10 ]LHRH. Its chemical structure is pyro-Glu-His-Trp-Ser-Tyr-D-Ser(Bu t )-Leu-Arg-Pro-Azgly-NH 2 acetate [C 59 H 84 N 18 O 14 ·(C 2 H 4 O 2 ) x where x = 1 to 2.4].
Goserelin acetate is an off-white powder with a molecular weight of 1269 Daltons (free base). It is freely soluble in glacial acetic acid. It is soluble in water, 0.1M hydrochloric acid, 0.1M sodium hydroxide, dimethylformamide and dimethyl sulfoxide. Goserelin acetate is practically insoluble in acetone, chloroform and ether.
ZOLADEX 10.8 mg implant is supplied as a sterile, biodegradable product containing goserelin acetate equivalent to 10.8 mg of goserelin. ZOLADEX is designed for subcutaneous implantation with continuous release over a 12-week period. Goserelin acetate is dispersed in a matrix of D,L-lactic and glycolic acids copolymer (12.82-14.76 mg/dose) containing less than 2% acetic acid and up to 10% goserelin-related substances and presented as a sterile, white to cream colored 1.5 mm diameter cylinder, preloaded in a special single-use syringe with a 14-gauge x 0.5 mm needle and protective needle sleeve (SafeSystem™ Syringe) in a sealed, light- and moisture-proof, aluminum foil laminate pouch containing a desiccant capsule.
Studies of the D,L-lactic and glycolic acids copolymer have indicated that it is completely biodegradable and has no demonstrable antigenic potential.
ZOLADEX is also supplied as a sterile, biodegradable product containing goserelin acetate equivalent to 3.6 mg of goserelin designed for administration every 28 days.
CLINICAL PHARMACOLOGY
Mechanism of Action: ZOLADEX is a synthetic decapeptide analogue of LHRH. ZOLADEX acts as a potent inhibitor of pituitary gonadotropin secretion when administered in the biodegradable formulation.
Following initial administration, ZOLADEX causes an initial increase in serum-luteinizing hormone (LH) and follicle-stimulating hormone (FSH) levels with subsequent increases in serum levels of testosterone. Chronic administration of ZOLADEX leads to sustained suppression of pituitary gonadotropins, and serum levels of testosterone consequently fall into the range normally seen in surgically castrated men approximately 21 days after initiation of therapy. This leads to accessory sex organ regression.
In animal and in in vitro studies, administration of goserelin resulted in the regression or inhibition of growth of the hormonally sensitive dimethylbenzanthracene (DMBA)-induced rat mammary tumor and Dunning R3327 prostate tumor.
In clinical trials using ZOLADEX 3.6 mg with follow-up of more than 2 years, suppression of serum testosterone to castrate levels has been maintained for the duration of therapy.
Pharmacokinetics:
Absorption: The pharmacokinetics of goserelin have been determined in healthy male volunteers and patients. In healthy males, radiolabeled goserelin was administered as a single 250 µg (aqueous solution) dose by the subcutaneous route. The absorption of radiolabeled drug was rapid, and the peak blood radioactivity levels occurred between 0.5 and 1.0 hour after dosing.
The overall pharmacokinetic profile of goserelin following administration of a ZOLADEX 10.8 mg depot to patients with prostate cancer was determined. The initial release of goserelin from the depot was relatively rapid resulting in a peak concentration at 2 hours after dosing. From Day 4 until the end of the 12-week dosing interval, the sustained release of goserelin from the depot produced reasonably stable systemic exposure. Mean (Standard Deviation) pharmacokinetic data are presented in Table 1. There is no clinically significant accumulation of goserelin following administration of four depots administered at 12-week intervals. Pharmacokinetic data were obtained using an RIA method, which has been shown to be specific for goserelin in the presence of its metabolites.
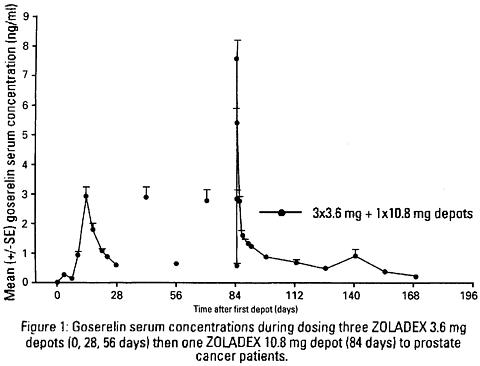
Table 1 Goserelin pharmacokinetic parameters for the 10.8 mg depot Parametern Mean (SD) 95% CI Lower Upper Systemic clearance (mL/min)41 121 (42.4) 108134C max (ng/mL)41 8.85 (2.83) 7.969.74T max (h)41 1.80 (0.34) 1.701.92C min (ng/mL)44 0.37 (0.21) 0.300.43Elimination Half-life (h) ¶7 4.16 (1.12) 3.125.20¶ = determined after subcutaneous administration of 250 µg aqueous solution of goserelin. SD = standard deviation 95% CI = 95% confidence interval Serum goserelin concentrations in prostate cancer patients administered three 3.6 mg depots followed by one 10.8 mg depot are displayed in Figure 1. The profiles for both formulations are primarily dependent upon the rate of drug release from the depots. For the 3.6 mg depot, mean concentrations gradually rise to reach a peak of about 3 ng/mL at around 15 days after administration and then decline to approximately 0.5 ng/mL by the end of the treatment period. For the 10.8 mg depot, mean concentrations increase to reach a peak of about 8 ng/mL within the first 24 hours and then decline rapidly up to Day 4. Thereafter, mean concentrations remain relatively stable in the range of about 0.3 to 1 ng/mL up to the end of the treatment period.
Administration of four ZOLADEX 10.8 mg depots to patients with prostate cancer resulted in testosterone levels that were suppressed to and maintained within the range normally observed in surgically castrated men (0-1.73 nmol/L or 0-50 ng/dL), over the dosing interval in approximately 91% (145/160) of patients studied. In 6 of 15 patients that escaped from castrate range, serum testosterone levels were maintained below 2.0 nmol/L (58 ng/dL) and in only one of the 15 patients did the depot completely fail to maintain serum testosterone levels to within the castrate range over a 336-day period (4 depot injections). In the 8 additional patients, a transient escape was followed 14 days later by a level within the castrate range.
Distribution: The apparent volume of distribution determined after subcutaneous administration of 250 µg aqueous solution of goserelin was 44.1 ± 13.6 liters for healthy males. The plasma protein binding of goserelin was found to be 27%.
Metabolism: Metabolism of goserelin, by hydrolysis of the C-terminal amino acids, is the major clearance mechanism. The major circulating component in serum appeared to be 1-7 fragment, and the major component present in urine of one healthy male volunteer was 5-10 fragment. The metabolism of goserelin in humans yields a similar but narrow profile of metabolites to that found in other species. All metabolites found in humans have also been found in toxicology species.
Excretion: Clearance of goserelin following subcutaneous administration of a radiolabeled solution of goserelin was very rapid and occurred via a combination of hepatic and urinary excretion. More than 90% of a subcutaneous radiolabeled solution formulation dose of goserelin was excreted in urine. Approximately 20% of the dose recovered in urine was accounted for by unchanged goserelin.
Special Populations
Renal Insufficiency: In clinical trials with the solution formulation of goserelin, subjects with impaired renal function (creatinine clearance less than 20 mL/min) had a serum elimination half-life of 12.1 hours compared to 4.2 hours for subjects with normal renal function (creatinine clearance greater than 70 mL/min). However, there was no evidence for any accumulation of goserelin on multiple dosing of the ZOLADEX 10.8 mg depot to subjects with impaired renal function. There was no evidence for any increase in incidence of adverse events in renally impaired patients administered the 10.8 mg depot. These data indicate that there is no need for any dosage adjustment when administering ZOLADEX 10.8 mg to subjects with impaired renal function.
Hepatic Insufficiency: The clearance and half-life of goserelin administered as an aqueous solution are not affected by hepatic impairment. These data indicate that there is no need for any dosage adjustment when administering ZOLADEX 10.8 mg to subjects with impaired hepatic function.
Geriatric: There is no need for any dosage adjustment when administering ZOLADEX 10.8 mg to geriatric patients.
Body Weight: A decline of approximately 1 to 2.5% in the AUC after administration of a 10.8 mg depot was observed with a kilogram increase in body weight. In obese patients who have not responded clinically, testosterone levels should be monitored closely.
Drug-Drug Interactions: No formal drug-drug interaction studies have been performed.
Clinical Studies--Prostatic Carcinoma: In two controlled clinical trials, 160 patients with advanced prostate cancer were randomized to receive either one 3.6 mg ZOLADEX implant every four weeks or a single 10.8 mg ZOLADEX implant every 12 weeks. Mean serum testosterone suppression was similar between the two arms. PSA falls at three months were 94% in patients who received the 10.8 mg implant and 92.5% in patients that received three 3.6 mg implants.
Periodic monitoring of serum testosterone levels should be considered if the anticipated clinical or biochemical response to treatment has not been achieved. A clinical outcome similar to that produced with the use of the 3.6 mg implant administered every 28 days is predicted with ZOLADEX 10.8 mg implant administered every 12 weeks (84 days). Total testosterone was measured by the DPC Coat-A-Count radioimmunoassay method which, as defined by the manufacturers, is highly specific and accurate. Acceptable variability of approximately 20% at low testosterone levels has been demonstrated in the clinical studies performed with the ZOLADEX 10.8 mg depot.
Clinical Studies--Stage B2-C Prostatic Carcinoma: The effects of hormonal treatment combined with radiation were studied in 466 patients (231 ZOLADEX + flutamide + radiation, 235 radiation alone) with bulky primary tumors confined to the prostate (stage B2) or extending beyond the capsule (stage C), with or without pelvic node involvement.
In this multicentered, controlled trial, administration of ZOLADEX (3.6 mg depot) and flutamide capsules (250 mg t.i.d.) prior to and during radiation was associated with a significantly lower rate of local failure compared to radiation alone (16% vs 33% at 4 years, P<0.001). The combination therapy also resulted in a trend toward reduction in the incidence of distant metastases (27% vs 36% at 4 years, P =0.058). Median disease-free survival was significantly increased in patients who received complete hormonal therapy combined with radiation as compared to those patients who received radiation alone (4.4 vs 2.6 years, P<0.001). Inclusion of normal PSA level as a criterion for disease-free survival also resulted in significantly increased median disease-free survival in patients receiving the combination therapy (2.7 vs 1.5 years, P<0.001).
INDICATIONS AND USAGE
Prostatic Carcinoma: ZOLADEX is indicated in the palliative treatment of advanced carcinoma of the prostate.
In controlled studies of patients with advanced prostatic cancer comparing ZOLADEX 3.6 mg to orchiectomy, the long-term endocrine responses and objective responses were similar between the two treatment arms. Additionally, duration of survival was similar between the two treatment arms in a major comparative trial.
In controlled studies of patients with advanced prostatic cancer, ZOLADEX 10.8 mg implant produced pharmacodynamically similar effect in terms of suppression of serum testosterone to that achieved with ZOLADEX 3.6 mg implant. Clinical outcome similar to that produced with the use of the ZOLADEX 3.6 mg implant administered every 28 days is predicted with the ZOLADEX 10.8 mg implant administered every 12 weeks.
Stage B2-C Prostatic Carcinoma: ZOLADEX is indicated for use in combination with flutamide for the management of locally confined Stage T2b-T4 (Stage B2-C) carcinoma of the prostate. Treatment with ZOLADEX and flutamide should start 8 weeks prior to initiating radiation therapy and continue during radiation therapy.
The automatic safety feature of the syringe aids in the prevention of needlestick injury.
CONTRAINDICATIONS
A report of an anaphylactic reaction to synthetic GnRH (Factrel) has been reported in the medical literature. ZOLADEX is contraindicated in those patients who have a known hypersensitivity to LHRH, LHRH agonist analogues or any of the components in ZOLADEX.
ZOLADEX 10.8 mg implant is not indicated in women as the data are insufficient to support reliable suppression of serum estradiol. For female patients requiring treatment with goserelin, refer to the prescribing information for ZOLADEX 3.6 mg implant.
ZOLADEX is contraindicated in women who are or may become pregnant while receiving the drug. In studies in rats and rabbits, ZOLADEX increased preimplantation loss, resorptions, and abortions (see Pregnancy section). In rats and dogs, ZOLADEX suppressed ovarian function, decreased ovarian weight and size, and led to atrophic changes in secondary sex organs. Further evidence suggests that fertility was reduced in female rats that became pregnant after ZOLADEX was stopped. These effects are an expected consequence of the hormonal alterations produced by ZOLADEX in humans. If a patient becomes pregnant during treatment, the drug must be discontinued and the patient must be apprised of the potential risk for loss of the pregnancy due to possible hormonal imbalance as a result of the expected pharmacologic action of ZOLADEX treatment. In animal studies, there was no evidence that ZOLADEX possessed the potential to cause teratogenicity in rabbits; however, in rats the incidence of umbilical hernia was significantly increased with treatment. (See Pregnancy, Teratogenic Effects .)
WARNINGS
Initially, ZOLADEX, like other LHRH agonists, causes transient increases in serum levels of testosterone. Transient worsening of symptoms, or the occurrence of additional signs and symptoms of prostatic cancer, may occasionally develop during the first few weeks of ZOLADEX treatment. A small number of patients may experience a temporary increase in bone pain, which can be managed symptomatically. As with other LHRH agonists, isolated cases of ureteral obstruction and spinal cord compression have been observed. If spinal cord compression or renal impairment develops, standard treatment of these complications should be instituted, and in extreme cases an immediate orchiectomy considered.
PRECAUTIONS
General: Hypersensitivity, antibody formation and acute anaphylactic reactions have been reported with LHRH agonist analogues.
Of 115 women worldwide treated with ZOLADEX 3.6 mg and tested for development of binding to goserelin following treatment with ZOLADEX, one patient showed low-titer binding to goserelin. On further testing of this patient's plasma obtained following treatment, her goserelin binding component was found not to be precipitated with rabbit antihuman immunoglobulin polyvalent sera. These findings suggest the possibility of antibody formation.
Information for Patients: The use of ZOLADEX in patients at particular risk of developing ureteral obstruction or spinal cord compression should be considered carefully and the patients monitored closely during the first month of therapy. Patients with ureteral obstruction or spinal cord compression should have appropriate treatment prior to initiation of ZOLADEX therapy.
Drug Interactions: No No drug interaction studies with other drugs have been conducted with ZOLADEX. No confirmed interactions have been reported between ZOLADEX and other drugs.
Drug/Laboratory Test Interactions: Administration of ZOLADEX in therapeutic doses results in suppression of the pituitary-gonadal system. Because of this suppression, diagnostic tests of pituitary-gonadotropic and gonadal functions conducted during treatment may show results which are misleading.
Carcinogenesis, Mutagenesis, Impairment of Fertility: Subcutaneous implant of ZOLADEX in male and female rats once every 4 weeks for 1 year and recovery for 23 weeks at doses of about 80 and 150 µg/kg (males) and 50 and 100 µg/kg (females) daily (about 3 to 9 times the recommended human dose on a mg/m 2 basis) resulted in an increased incidence of pituitary adenomas. An increased incidence of pituitary adenomas was also observed following subcutaneous implant of ZOLADEX in rats at similar dose levels for a period of 72 weeks in males and 101 weeks in females. The relevance of the rat pituitary adenomas to humans has not been established. Subcutaneous implants of ZOLADEX every 3 weeks for 2 years delivered to mice at doses of up to 2400 µg/kg/day (about 70 times the recommended human dose on a mg/m 2 basis) resulted in an increased incidence of histiocytic sarcoma of the vertebral column and femur.
Mutagenicity tests using bacterial and mammalian systems for point mutations and cytogenetic effects have provided no evidence for mutagenic potential.
Administration of goserelin led to changes that were consistent with gonadal suppression in both male and female rats as a result of its endocrine action. In male rats administered 500-1000 µg/kg/day (about 30-60 times the recommended human dose on a mg/m 2 basis), a decrease in weight and atrophic histological changes were observed in the testes, epididymis, seminal vesicle and prostate gland with complete suppression of spermatogenesis. In female rats administered 50-1000 µg/kg/day (about 3-60 times the recommended daily human dose on a mg/m 2 basis), suppression of ovarian function led to decreased size and weight of ovaries and secondary sex organs; follicular development was arrested at the antral stage and the corpora lutea were reduced in size and number. Except for the testes, almost complete histologic reversal of these effects in males and females was observed several weeks after dosing was stopped; however, fertility and general reproductive performance were reduced in those that became pregnant after goserelin was discontinued. Fertile matings occurred within 2 weeks after cessation of dosing, even though total recovery of reproductive function may not have occurred before mating took place; and, the ovulation rate, the corresponding implantation rate, and number of live fetuses were reduced.
Based on histological examination, drug effects on reproductive organs seem to be completely reversible in male and female dogs when drug treatment was stopped after continuous administration for 1 year at 100 times the recommended monthly dose.
Pregnancy, Teratogenic Effects: Pregnancy Category X. See CONTRAINDICATIONS section. ZOLADEX 10.8 mg is not indicated in women as the data are insufficient to support reliable suppression of serum estradiol. Studies in both rats and rabbits at doses of 2, 10, 20, and 50 µg/kg/day and 20, 250, and 1,000 µg/kg/day, respectively (about 1/10 to 3 times and 2 to 100 times the daily maximum recommended human dose, respectively, on a mg/m 2 basis) administered during the period of organogenesis, have confirmed that ZOLADEX will increase pregnancy loss in a dose-related manner. While there was no evidence that ZOLADEX possessed the potential to cause teratogenicity in rabbits, in rats the incidence of umbilical hernia was significantly increased at doses greater than 10 mg/kg/day (about 1/2 the recommended dose on a mg/m 2 basis).
Nursing Mothers: It is not known if this drug is excreted in human milk. Many drugs are excreted in human milk and there is a potential for serious adverse reactions in nursing infants of mothers receiving ZOLADEX (See CONTRAINDICATIONS ).
Pediatric Use: Safety and efficacy of ZOLADEX in pediatric patients have not been established.
ADVERSE REACTIONS
General: Rarely, hypersensitivity reactions (including urticaria and anaphylaxis) have been reported in patients receiving ZOLADEX.
As with other endocrine therapies, hypercalcemia (increased calcium) has rarely been reported in cancer patients with bone metastases following initiation of treatment with ZOLADEX or other LHRH agonists.
ZOLADEX has been found to be generally well tolerated in clinical trials. Adverse reactions reported in these trials were rarely severe enough to result in the patients' withdrawal from ZOLADEX treatment. As seen with other hormonal therapies, the most commonly observed adverse events during ZOLADEX therapy were due to the expected physiological effects from decreased testosterone levels. These included hot flashes, sexual dysfunction and decreased erections.
As with other agents in this class, very rare cases of pituitary apoplexy have been reported following initial administration in patients with a functional pituitary adenoma.
Initially, ZOLADEX, like other LHRH agonists, causes transient increases in serum levels of testosterone. A small percentage of patients experienced a temporary worsening of signs and symptoms (see WARNINGS section), usually manifested by an increase in cancer-related pain which was managed symptomatically. Isolated cases of exacerbation of disease symptoms, either ureteral obstruction or spinal cord compression, occurred at similar rates in controlled clinical trials with both ZOLADEX and orchiectomy. The relationship of these events to therapy is uncertain.
There have been post-marketing reports of osteoporosis, decreased bone mineral density and bony fracture in men treated with ZOLADEX for prostate cancer.
Changes in blood pressure, manifest as hypotension or hypertension, have been occasionally observed in patients administered ZOLADEX. The changes are usually transient, resolving either during continued therapy or after cessation of therapy with ZOLADEX. Rarely, such changes have been sufficient to require medical intervention including withdrawal of treatment from ZOLADEX.
Prostatic Carcinoma: Two controlled clinical trials using ZOLADEX 10.8 mg versus ZOLADEX 3.6 mg were conducted. During a comparative phase, patients were randomized to receive either a single 10.8 mg implant or three consecutive 3.6 mg implants every 4 weeks over weeks 0-12. During this phase, the only adverse event reported in greater than 5% of patients was hot flashes, with an incidence of 47% in the ZOLADEX 10.8 mg group and 48% in the ZOLADEX 3.6 mg group.
From weeks 12-48 all patients were treated with a 10.8 mg implant every 12 weeks. During this noncomparative phase, the following adverse events were reported in greater than 5% of patients:
Adverse EventZOLADEX 10.8 mg
(n = 157)
%Hot Flashes64 Pain (General)14 Gynecomastia8 Pelvic Pain6 Bone Pain6 Asthenia5 The following adverse events were reported in greater than 1%, but less than 5% of patients treated with ZOLADEX 10.8 mg implant every 12 weeks. Some of these are commonly reported in elderly patients.
WHOLE BODY--Abdominal pain, Back pain, Flu syndrome, Headache, Sepsis, Aggravation reaction
CARDIOVASCULAR--Angina pectoris, Cerebral ischemia, Cerebrovascular accident, Heart failure, Pulmonary embolus, Varicose veins
DIGESTIVE--Diarrhea, Hematemesis
ENDOCRINE--Diabetes mellitus
HEMATOLOGIC--Anemia
METABOLIC--Peripheral edema
NERVOUS SYSTEM--Dizziness, Paresthesia, Urinary retention
RESPIRATORY--Cough increased, Dyspnea, Pneumonia
SKIN--Herpes simplex, Pruritus
UROGENITAL--Bladder neoplasm, Breast pain, Hematuria, Impotence, Urinary frequency, Urinary incontinence, Urinary tract disorder, Urinary tract infection, Urination impaired.
The following adverse events not already listed above were reported in patients receiving ZOLADEX 3.6 mg in other clinical trials. Inclusion does not necessarily represent a causal relationship to ZOLADEX 10.8 mg.
WHOLE BODY: Allergic reaction, Chills, Fever, Infection, Injection site reaction, Lethargy, Malaise
CARDIOVASCULAR: Arrhythmia, Chest pain, Hemorrhage, Hypertension, Migraine, Myocardial infarction, Palpitations, Peripheral vascular disorder, Tachycardia
DIGESTIVE: Anorexia, Constipation, Dry mouth, Dyspepsia, Flatulence, Increased appetite, Nausea, Ulcer, Vomiting
HEMATOLOGIC: Ecchymosis
METABOLIC: Edema, Gout, Hyperglycemia, Weight increase
MUSCULOSKELETAL: Arthralgia, Hypertonia, Joint disorder, Leg cramps, Myalgia, Osteoporosis
NERVOUS SYSTEM: Anxiety, Depression, Emotional lability, Headache, Insomnia, Nervousness, Somnolence, Thinking abnormal
RESPIRATORY: Bronchitis, Chronic obstructive pulmonary disease, Epistaxis, Rhinitis, Sinusitis, Upper respiratory infection, Voice alterations
SKIN: Acne, Alopecia, Dry skin, Hair disorders, Rash, Seborrhea, Skin discoloration, Sweating
SPECIAL SENSES: Amblyopia, Dry eyes
UROGENITAL: Breast tenderness, Decreased erections, Renal insufficiency, Sexual dysfunction, Urinary obstruction
Stage B2-C Prostatic Carcinoma: Treatment with ZOLADEX and flutamide did not add substantially to the toxicity of radiation treatment alone. The following adverse experiences were reported during a multicenter clinical trial comparing ZOLADEX + flutamide + radiation versus radiation alone. The most frequently reported (greater than 5%) adverse experiences are listed below:
ADVERSE EVENTS DURING ACUTE
RADIATION THERAPY
(within first 90 days of radiation therapy)(n=231)
flutamide +
ZOLADEX +
Radiation
% All(n=235)
Radiation Only
% AllRectum/Large
Bowel80 76 Bladder58 60 Skin37 37 ADVERSE EVENTS DURING LATE RADIATION PHASE
(after 90 days of radiation therapy)(n=231)
flutamide +
ZOLADEX +
Radiation
% All(n=235)
Radiation Only
% AllDiarrhea36 40 Cystitis16 16 Rectal Bleeding14 20 Proctitis8 8 Hematuria7 12 Additional adverse event data was collected for the combination therapy with radiation group over both the hormonal treatment and hormonal treatment plus radiation phases of the study. Adverse experiences occurring in more than 5% of patients in this group, over both parts of the study, were hot flashes (46%), diarrhea (40%), nausea (9%), and skin rash (8%).
Changes in Laboratory Values During Treatment
Plasma Enzymes: Elevation of liver enzymes (AST, ALT) have been reported in female patients exposed to ZOLADEX 3.6 mg (representing less than 1% of all patients). There was no other evidence of abnormal liver function. Causality between these changes and ZOLADEX have not been established.
Lipids: In a controlled trial in females, ZOLADEX 3.6 mg implant therapy resulted in a minor, but statistically significant effect on serum lipids (i.e., increases in LDL cholesterol of 21.3 mg/dL; increases in HDL cholesterol of 2.7 mg/dL; and triglycerides increased by 8.0 mg/dL).
OVERDOSAGE
The pharmacologic properties of ZOLADEX and its mode of administration make accidental or intentional overdosage unlikely. There is no experience of overdosage from clinical trials. Animal studies indicate that no increased pharmacologic effect occurred at higher doses or more frequent administration. Subcutaneous doses of the drug as high as 1 mg/kg/day in rats and dogs did not produce any nonendocrine related sequelae; this dose is greater than 400 times that proposed for human use. If overdosage occurs, it should be managed symptomatically.
DOSAGE AND ADMINISTRATION
ZOLADEX, at a dose of 10.8 mg, should be administered subcutaneously every 12 weeks into the anterior abdominal wall below the navel line using an aseptic technique under the supervision of a physician.
While a delay of a few days is permissible, every effort should be made to adhere to the 12-week schedule.
Prostatic Carcinoma: For the management of advanced prostate cancer, ZOLADEX is intended for long-term administration unless clinically inappropriate.
Stage B2-C Prostatic Carcinoma: When ZOLADEX is given in combination with radiotherapy and flutamide for patients with Stage T2b-T4 (Stage B2-C) prostatic carcinoma, treatment should be started 8 weeks prior to initiating radiotherapy and should continue during radiation therapy. A treatment regimen using one ZOLADEX 3.6 mg depot, followed in 28 days by one ZOLADEX 10.8 mg depot, should be administered.
Renal or Hepatic Impairment: No dosage adjustment is necessary for patients with renal or hepatic impairment.
Females: ZOLADEX 10.8 mg implant is not indicated in women as the data are insufficient to support reliable suppression of serum estradiol. For female patients requiring treatment with goserelin, refer to the prescribing information for ZOLADEX 3.6 mg implant.
Administration Technique: The proper method of administration of ZOLADEX is described in the instructions that follow.
- Put the patient in a comfortable position with the upper part of the body slightly raised. Prepare an area of the anterior abdominal wall below the navel line with an alcohol swab.
- Examine the foil pouch and syringe for damage. Remove the syringe from the opened foil pouch and hold the syringe at a slight angle to the light. Check that at least part of the ZOLADEX implant is visible.
- Grasp the blue plastic safety tab and pull away from the syringe, and discard. Remove needle cover. Unlike liquid injections, there is no need to remove air bubbles as attempts to do so may displace the ZOLADEX implant.
-
Holding the syringe around the protective sleeve, using an aseptic technique, pinch the skin of the patient's anterior abdominal wall below the navel line. With the bevel of the needle facing up,
insert the needle at a 30 to 45 degree angle to the skin in one continuous deliberate motion until the protective sleeve touches the patient's skin (Figure 3).
NOTE: The ZOLADEX syringe cannot be used for aspiration. If the hypodermic needle penetrates a large vessel, blood will be seen instantly in the syringe chamber. If a vessel is penetrated, withdraw the needle and inject with a new syringe elsewhere. - Do not penetrate into muscle or peritoneum.
-
To administer the ZOLADEX implant and to activate the protective sleeve, grasp the barrel at the finger grip and depress the plunger until you cannot depress it any further. If the plunger is not depressed
fully
the protective sleeve will
NOT
activate. When the protective sleeve 'clicks', the protective sleeve will automatically begin to slide to cover the needle.
NOTE: The needle does not retract. -
Withdraw the needle and allow protective sleeve to slide and cover needle. Dispose of the syringe in an approved sharps collector.
NOTE: In the unlikely event of the need to surgically remove ZOLADEX, it may be localized by ultrasound.
HOW SUPPLIED
ZOLADEX 10.8 mg implant is supplied as a sterile and totally biodegradable D,L-lactic and glycolic acids copolymer (12.82-14.76 mg/dose) impregnated with goserelin acetate equivalent to 10.8 mg of goserelin in a disposable syringe device fitted with a 14-gauge x 0.5 mm hypodermic needle with protective needle sleeve [SafeSystem™ Syringe] (NDC 0310-0951-30). The unit is sterile and comes in a sealed, light- and moisture-proof, aluminum foil laminate pouch containing a desiccant capsule. Store at room temperature (do not exceed 25°C [77°F]).
ZOLADEX is a trademark of the Astrazeneca group of companies.
©Astrazeneca 2002, 2003
Manufactured for:
Astrazeneca Pharmaceuticals LP
Wilmington, DE 19850
by Astrazeneca UK Limited
Macclesfield, England
Made in the United Kingdom
64225-00
Rev 03/04
Subscribe to the "News" RSS Feed 
TOP ۞