-
Nutropin AQ Injection, Nutropin AQ Pen, Nutropin AQ Pen Cartridge (Genentech)
DESCRIPTION
Nutropin AQ is a human growth hormone (hGH) produced by recombinant DNA technology. Nutropin AQ has 191 amino acid residues and a molecular weight of 22,125 daltons. The amino acid sequence of the product is identical to that of pituitary-derived human growth hormone. The protein is synthesized by a specific laboratory strain of E. coli as a precursor consisting of the rhGH molecule preceded by the secretion signal from an E. coli protein. This precursor is directed to the plasma membrane of the cell. The signal sequence is removed and the native protein is secreted into the periplasm so that the protein is folded appropriately as it is synthesized.
Nutropin AQ is a highly purified preparation. Biological potency is determined using a cell proliferation bioassay. Nutropin AQ may contain not more than fifteen percent deamidated growth hormone (GH) at expiration. The de-amidated form of GH has been extensively characterized and has been shown to be safe and fully active.
Nutropin AQ is a sterile liquid intended for subcutaneous administration. The product is nearly isotonic at a concentration of 5 mg of GH per mL and has a pH of approximately 6.0.
The Nutropin AQ 2 mL vial contains 10 mg (approximately 30 International Units [IU]) somatropin, formulated in 17.4 mg sodium chloride, 5 mg phenol, 4 mg polysorbate 20, and 10 mM sodium citrate.
The Nutropin AQ 2 mL pen cartridge contains 10 mg (approximately 30 International Units) somatropin, formulated in 17.4 mg sodium chloride, 5 mg phenol, 4 mg polysorbate 20, and 10 mM sodium citrate.
CLINICAL PHARMACOLOGY
General
In vitro and in vivo preclinical and clinical testing have demonstrated that Nutropin AQ is therapeutically equivalent to pituitary-derived human GH (hGH). Pediatric patients who lack adequate endogenous GH secretion, patients with chronic renal insufficiency, and patients with Turner syndrome that were treated with Nutropin AQ or Nutropin ® [somatropin (rDNA origin) for injection] resulted in an increase in growth rate and an increase in insulin-like growth factor-I (IGF-I) levels similar to that seen with pituitary-derived hGH.
Actions that have been demonstrated for Nutropin AQ, somatropin, somatrem, and/or pituitary-derived hGHinclude:
-
Tissue Growth
1) Skeletal Growth: GH stimulates skeletal growth in pediatric patients with growth failure due to a lack of adequate secretion of endogenous GH or secondary to chronic renal insufficiency and in patients with Turner syndrome. Skeletal growth is accomplished at the epiphyseal plates at the ends of a growing bone. Growth and metabolism of epiphyseal plate cells are directly stimulated by GH and one of its mediators, IGF-I. Serum levels of IGF-I are low in children and adolescents who are GH deficient, but increase during treatment with GH. In pediatric patients, new bone is formed at the epiphyses in response to GH and IGF-I. This results in linear growth until these growth plates fuse at the end of puberty. 2) Cell Growth: Treatment with hGH results in an increase in both the number and the size of skeletal muscle cells. 3) Organ Growth: GH influences the size of internal organs, including kidneys, and increases red cell mass. Treatment of hypophysectomized or genetic dwarf rats with GH results in organ growth that is proportional to the overall body growth. In normal rats subjected to nephrectomy-induced uremia, GH promoted skeletal and body growth. -
Protein Metabolism
Linear growth is facilitated in part by GH-stimulated protein synthesis. This is reflected by nitrogen retention as demonstrated by a decline in urinary nitrogen excretion and blood urea nitrogen during GH therapy. -
Carbohydrate Metabolism
GH is a modulator of carbohydrate metabolism. For example, patients with inadequate secretion of GH sometimes experience fasting hypoglycemia that is improved by treatment with GH. GH therapy may decrease insulin sensitivity. Untreated patients with chronic renal insufficiency and Turner syndrome have an increased incidence of glucose intolerance. Administration of hGH to adults or children resulted in increases in serum fasting and postprandial insulin levels, more commonly in overweight or obese individuals. In addition, mean fasting and postprandial glucose and hemoglobin A 1c levels remained in the normal range. -
Lipid Metabolism
In GH-deficient patients, administration of GH resulted in lipid mobilization, reduction in body fat stores, increased plasma fatty acids, and decreased plasma cholesterol levels. -
Mineral Metabolism
The retention of total body potassium in response to GH administration apparently results from cellular growth. Serum levels of inorganic phosphorus may increase slightly in patients with inadequate secretion of endogenous GH, chronic renal insufficiency, or patients with Turner syndrome during GH therapy due to metabolic activity associated with bone growth as well as increased tubular reabsorption of phosphate by the kidney. Serum calcium is not significantly altered in these patients. Sodium retention also occurs. Adults with childhood-onset GH deficiency show low bone mineral density (BMD). GH therapy results in increases in serum alkaline phosphatase. (See PRECAUTIONS : Laboratory Tests ). -
Connective Tissue Metabolism
GH stimulates the synthesis of chondroitin sulfate and collagen as well as the urinary excretion of hydroxyproline.
Pharmacokinetics
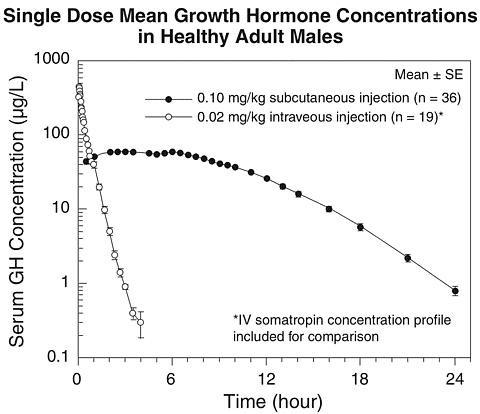
Subcutaneous Absorption --The absolute bioavailability of recombinant human growth hormone (rhGH) after subcutaneous administration in healthy adult males has been determined to be 81 ± 20%. The mean terminal t ½ after subcutaneous administration is significantly longer than that seen after intravenous administration (2.1 ± 0.43 hr vs. 19.5 ± 3.1 min) indicating that the subcutaneous absorption of the compound is slow and rate-limiting.
Distribution --Animal studies with rhGH showed that GH localizes to highly perfused organs, particularly the liver and kidney. The volume of distribution at steady state for rhGH in healthy adult males is about 50 mL/kg body weight, approximating the serum volume.
Metabolism --Both the liver and kidney have been shown to be important metabolizing organs for GH. Animal studies suggest that the kidney is the dominant organ of clearance. GH is filtered at the glomerulus and reabsorbed in the proximal tubules. It is then cleaved within renal cells into its constituent amino acids, which return to the systemic circulation.
Elimination --The mean terminal t ½ after intravenous administration of rhGH in healthy adult males is estimated to be 19.5 ± 3.1 minutes. Clearance of rhGH after intravenous administration in healthy adults and children is reported to be in the range of 116-174 mL/hr/kg.
Bioequivalence of Formulations --Nutropin AQ has been determined to be bioequivalent to Nutropin based on the statistical evaluation of AUC and C max .
SPECIAL POPULATIONS
Pediatric --Available literature data suggest that rhGH clearances are similar in adults and children.
Gender --No data are available for exogenously administered rhGH. Available data for methionyl recombinant GH, pituitary-derived GH, and endogenous GH suggest no consistent gender-based differences in GH clearance.
Geriatrics --Limited published data suggest that the plasma clearance and average steady-state plasma concentration of rhGH may not be different between young and elderly patients.
Race --Reported values for half-lives for endogenous GH in normal adult black males are not different from observed values for normal adult white males. No data for other races are available.
Growth Hormone Deficiency (GHD) --Reported values for clearance of rhGH in adults and children with GHD range 138-245 mL/hr/kg and are similar to those observed in healthy adults and children. Mean terminal t ½ values following intravenous and subcutaneous administration in adult and pediatric GHD patients are also similar to those observed in healthy adult males.
Renal Insufficiency --Children and adults with chronic renal failure (CRF) and end-stage renal disease (ESRD) tend to have decreased clearance compared to normal individuals. Endogenous GH production may also increase in some individuals with ESRD. However, no rhGH accumulation has been reported in children with CRF or ESRD dosed with current regimens.
Turner Syndrome --No pharmacokinetic data are available for exogenously administered rhGH. However, reported half-lives, absorption, and elimination rates for endogenous GH in this population are similar to the ranges observed for normal subjects and GHD populations.
Hepatic Insufficiency --A reduction in rhGH clearance has been noted in patients with severe liver dysfunction. The clinical significance of this decrease is unknown.
Summary of Nutropin AQ Pharmacokinetic Parameters
in Healthy Adult Males
0.1 mg (approximately 0.3 IU a )/kg SCC max
(µg/L)T max
(hr)t ½
(hr)AUC 0-(infinity)
(µg·hr/L)CL/F sc
(mL/[hr·kg])MEAN b71.1 3.9 2.3 677 150 CV%17 56 18 13 13 Abbreviations:C max =maximum concentrationt ½ =half-lifeAUC 0-(infinity) =area under the curveCL/F sc =systemic clearanceF sc =subcutaneous bioavailability (not determined)CV%=coefficient of variation in %; SC=subcutaneousa Based on current International Standard of 3 IU=1 mgb n=36
EFFICACY STUDIES
Growth Hormone Deficiency (GHD) in Pubertal Patients
One open label, multicenter, randomized clinical trial of two dosages of Nutropin ® [somatropin (rDNA origin) for injection] was performed in pubertal patients with GHD. Ninety-seven patients (mean age 13.9 years, 83 male, 14 female) currently being treated with approximately 0.3 mg/kg/wk of GH were randomized to 0.3 mg/kg/wk or 0.7 mg/kg/wk Nutropin doses. All patients were already in puberty (Tanner stage >/= 2) and had bone ages </= 14 years in males or </=12 years in females. Mean baseline height standard deviation (SD) score was -1.3.
The mean last measured height in all 97 patients after a mean duration of 2.7 ± 1.2 years, by analysis of covariance (ANCOVA) adjusting for baseline height, is shown below.
Last Measured Height * by Sex and Nutropin Dose Last Measured Height * (cm) Age (yr) 0.3 mg/kg/wk 0.7 mg/kg/wk Height Difference
Between Groups (cm)Mean±SD
(range)Mean±SD Mean±SD Mean±SE Male17.2±1.3
(13.6 to 19.4)170.9±7.9
(n=42)174.5±7.9
(n=41)3.6±1.7 Female15.8±1.8
(11.9 to 19.3)154.7±6.3
(n=7)157.6±6.3
(n=7)2.9±3.4 *Adjusted for baseline height
The mean height SD score at last measured height (n = 97) was -0.7 ± 1.0 in the 0.3 mg/kg/wk group and -0.1 ± 1.2 in the 0.7 mg/kg/wk group. For patients completing 3.5 or more years (mean 4.1 years) of Nutropin treatment (15/49 patients in the 0.3 mg/kg/wk group and 16/48 patients in the 0.7 mg/kg/wk group), the mean last measured height was 166.1 ± 8.0 cm in the 0.3 mg/kg/wk group and 171.8 ± 7.1 cm in the 0.7 mg/kg/wk group, adjusting for baseline height and sex.
The mean change in bone age was approximately one year for each year in the study in both dose groups. Patients with baseline height SD scores above -1.0 were able to attain normal adult heights with the 0.3 mg/kg/wk dose of Nutropin (mean height SD score at near-adult height = -0.1, n = 15).
Thirty-one patients had bone mineral density (BMD) determined by dual energy x-ray absorptiometry (DEXA) scans at study conclusion. The two dose groups did not differ significantly in mean SD score for total body BMD (-0.9 ± 1.9 in the 0.3 mg/kg/wk group vs. -0.8 ± 1.2 in the 0.7 mg/kg/wk group, n = 20) or lumbar spine BMD (-1.0 ± 1.0 in the 0.3 mg/kg/wk group vs. -0.2 ± 1.7 in the 0.7 mg/kg/wk group, n = 21).
Over a mean duration of 2.7 years, patients in the 0.7 mg/kg/wk group were more likely to have IGF-I values above the normal range than patients in the 0.3 mg/kg/wk group (27.7% vs. 9.0% of IGF-I measurements for individual patients). The clinical significance of elevated IGF-I values is unknown.
Effects of Nutropin on Growth Failure Due to Chronic Renal Insufficiency (CRI)
Two multicenter, randomized, controlled clinical trials were conducted to determine whether treatment with Nutropin prior to renal transplantation in patients with chronic renal insufficiency could improve their growth rates and height deficits. One study was a double-blind, placebo-controlled trial and the other was an open-label, randomized trial. The dose of Nutropin in both controlled studies was 0.05 mg/kg/day (0.35 mg/kg/week) administered daily by subcutaneous injection. Combining the data from those patients completing two years in the two controlled studies results in 62 patients treated with Nutropin and 28 patients in the control groups (either placebo-treated or untreated). The mean first year growth rate was 10.8 cm/yr for Nutropin-treated patients, compared with a mean growth rate of 6.5 cm/yr for placebo/untreated controls (p < 0.00005). The mean second year growth rate was 7.8 cm/yr for the Nutropin-treated group, compared with 5.5 cm/yr for controls (p < 0.00005). There was a significant increase in mean height standard deviation (SD) score in the Nutropin group (-2.9 at baseline to -1.5 at Month 24, n = 62) but no significant change in the controls (-2.8 at baseline to -2.9 at Month 24, n = 28). The mean third year growth rate of 7.6 cm/yr in the Nutropin-treated patients (n = 27) suggests that Nutropin stimulates growth beyond two years. However, there are no control data for the third year because control patients crossed over to Nutropin treatment after two years of participation. The gains in height were accompanied by appropriate advancement of skeletal age. These data demonstrate that Nutropin therapy improves growth rate and corrects the acquired height deficit associated with chronic renal insufficiency. Currently there are insufficient data regarding the benefit of treatment beyond three years. Although predicted final height was improved during Nutropin therapy, the effect of Nutropin on final adult height remains to be determined.
Post-Transplant Growth
The North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) has reported data for growth post-transplant in children who did not receive GH. The average change in height SD score during the initial two years post-transplant was 0.18 (n = 300, J Pediatr . 1993;122:397-402).
Controlled studies of GH treatment for the short stature associated with CRI were not designed to compare the growth of treated or untreated patients after they received renal transplants. However, growth data are available from a small number of patients who have been followed for at least 11 months. Of the 7 control patients, 4 increased their height SD score and 3 had either no significant change or a decrease in height SD score. The 13 patients treated with Nutropin prior to transplant had either no significant change or an increase in height SD score after transplantation, indicating that the individual gains achieved with GH therapy prior to transplant were maintained after transplantation. The differences in the height deficit narrowed between the treated and untreated groups in the post-transplant period.
Turner Syndrome
One long-term, randomized, open-label, multicenter, concurrently controlled study, two long-term, open-label, multicenter, historically controlled studies, and one long-term, randomized, dose-response study were conducted to evaluate the efficacy of GH for the treatment of girls with short stature due to Turner syndrome.
In the randomized study GDCT, comparing GH-treated patients to a concurrent control group who received no GH, the GH-treated patients who received a dose of 0.3 mg/kg/week given 6 times per week from a mean age of 11.7 years for a mean duration of 4.7 years attained a mean near final height of 146.0 cm (n = 27) as compared to the control group who attained a near final height of 142.1 cm (n = 19). By analysis of covariance, the effect of GH therapy was a mean height increase of 5.4 cm (p = 0.001).
In two of the studies (85-023 and 85-044), the effect of long-term GH treatment (0.375 mg/kg/week given either 3 times per week or daily) on adult height was determined by comparing adult heights in the treated patients with those of age-matched historical controls with Turner syndrome who never received any growth-promoting therapy. In Study 85-023, estrogen treatment was delayed until patients were at least age 14. GH therapy resulted in a mean adult height gain of 7.4 cm (mean duration of GH therapy of 7.6 years) vs. matched historical controls by analysis of covariance.
In Study 85-044, patients treated with early GH therapy were randomized to receive estrogen-replacement therapy (conjugated estrogens, 0.3 mg escalating to 0.625 mg daily) at either age 12 or 15 years. Compared with matched historical controls, early GH therapy (mean duration of GH therapy 5.6 years) combined with estrogen replacement at age 12 years resulted in an adult height gain of 5.9 cm (n = 26), whereas girls who initiated estrogen at age 15 years (mean duration of GH therapy 6.1 years) had a mean adult height gain of 8.3 cm (n = 29). Patients who initiated GH therapy after age 11 (mean age 12.7 years; mean duration of GH therapy 3.8 years) had a mean adult height gain of 5.0 cm (n = 51).
Thus, in both studies, 85-023 and 85-044, the greatest improvement in adult height was observed in patients who received early GH treatment and estrogen after age 14 years.
In a randomized, blinded, dose-response study, GDCI, patients were treated from a mean age of 11.1 years for a mean duration of 5.3 years with a weekly dose of either 0.27 mg/kg or 0.36 mg/kg administered 3 or 6 times weekly. The mean near final height of patients receiving growth hormone was 148.7 cm (n = 31). This represents a mean gain in adult height of approximately 5 cm compared with previous observations of untreated Turner syndrome girls.
In these studies, Turner syndrome patients (n = 181) treated to final adult height achieved statistically significant average estimated adult height gains ranging from 5.0-8.3 cm.
Study/
GroupStudy
Design aN at Adult
HeightGH Age
(yr)Estrogen Age
(yr)GH Duration
(yr)Adult Height
Gain (cm) bGDCTRCT 27 11.7 13 4.7 5.4 85-023MHT 17 9.1 15.2 7.6 7.4 85-044: A *MHT 29 9.4 15.0 6.1 8.3 B *26 9.6 12.3 5.6 5.9 C *51 12.7 13.7 3.8 5.0 GDCIRDT 31 11.1 8-13.5 5.3 ~5 c a RCT: randomized controlled trial; MHT: matched historical controlled trial;
RDT: randomized dose-response trial.b Analysis of covariance vs. controlsc Compared with historical data* A = GH age <11 yr, estrogen age 15 yr
B = GH age <11 yr, estrogen age 12 yr
C = GH age >11 yr, estrogen at Month 12Adult Growth Hormone Deficiency (GHD)
Two multicenter, double-blind, placebo-controlled clinical trials were conducted using Nutropin ® [somatropin (rDNA origin) for injection] in GH-deficient adults. One study was conducted in subjects with adult-onset GHD, mean age 48.3 years, n = 166, at doses of 0.0125 or 0.00625 mg/kg/day; doses of 0.025 mg/kg/day were not tolerated in these subjects. A second study was conducted in previously treated subjects with childhood-onset GHD, mean age 23.8 years, n = 64, at randomly assigned doses of 0.025 or 0.0125 mg/kg/day. The studies were designed to assess the effects of replacement therapy with GH on body composition.
Significant changes from baseline to Month 12 of treatment in body composition (i.e., total body % fat mass, trunk % fat mass, and total body % lean mass by DEXA scan) were seen in all Nutropin groups in both studies (p<0.0001 for change from baseline and vs. placebo), whereas no statistically significant changes were seen in either of the placebo groups. In the adult-onset study, the Nutropin group improved mean total body fat from 35.0% to 31.5%, mean trunk fat from 33.9% to 29.5%, and mean lean body mass from 62.2% to 65.7%, whereas the placebo group had mean changes of 0.2% or less (p = not significant). Due to the possible effect of GH-induced fluid retention on DEXA measurements of lean body mass, DEXA scans were repeated approximately 3 weeks after completion of therapy; mean % lean body mass in the Nutropin group was 65.0%, a change of 2.8% from baseline, compared with a change of 0.4% in the placebo group (p<0.0001 between groups).
In the childhood-onset study, the high-dose Nutropin group improved mean total body fat from 38.4% to 32.1%, mean trunk fat from 36.7% to 29.0%, and mean lean body mass from 59.1% to 65.5%; the low-dose Nutropin group improved mean total body fat from 37.1% to 31.3%, mean trunk fat from 37.9% to 30.6%, and mean lean body mass from 60.0% to 66.0%; the placebo group had mean changes of 0.6% or less (p = not significant).
Mean Changes from Baseline to Month 12 in Proportion of Fat and
Lean by DEXA for Studies M0431g and M0381g
(Adult-onset and Childhood-onset GHD, respectively)M0431g M0381g ProportionPlacebo
(n=62)Nutropin
(n=63)Between-Groups
t-test
p-valuePlacebo
(n=13)Nutropin
0.0125 mg/kg/day
(n=15)Nutropin
0.025 mg/kg/day
(n=15)Placebo vs.
Pooled Nutropin
t-test p-valueTotal body percent fatBaseline36.8 35.0 0.38 35.0 37.1 38.4 0.45 Month 1236.8 31.5 35.2 31.3 32.1 Baseline to Month 12 change-0.1 -3.6 <0.0001 +0.2 -5.8 -6.3 <0.0001 Post-washout36.4 32.2 NA NA NA Baseline to post-washout change-0.4 -2.8 <0.0001 NA NA NA Trunk percent fatBaseline35.3 33.9 0.50 32.5 37.9 36.7 0.23 Month 1235.4 29.5 33.1 30.6 29.0 Baseline to Month 12 change0.0 -4.3 <0.0001 +0.6 -7.3 -7.6 <0.0001 Post-washout34.9 30.5 NA NA NA Baseline to post-washout change-0.3 -3.4 NA NA NA Total body percent leanBaseline60.4 62.2 0.37 62.0 60.0 59.1 0.48 Month 1260.5 65.7 61.8 66.0 65.5 Baseline to Month 12 change+0.2 +3.6 <0.0001 -0.2 +6.0 +6.4 <0.0001 Post-washout60.9 65.0 NA NA NA Baseline to post-washout change+0.4 +2.8 <0.0001 NA NA NA In the adult-onset study, significant decreases from baseline to Month 12 in LDL cholesterol and LDL:HDL ratio were seen in the Nutropin group compared to the placebo group, p<0.02; there were no statistically significant between-group differences in change from baseline to Month 12 in total cholesterol, HDL cholesterol, or triglycerides. In the childhood-onset study, significant decreases from baseline to Month 12 in total cholesterol, LDL cholesterol, and LDL:HDL ratio were seen in the high-dose Nutropin group only, compared to the placebo group, p<0.05. There were no statistically significant between-group differences in HDL cholesterol or triglycerides from baseline to Month 12.
In the childhood-onset study, 55% of the patients had decreased spine bone mineral density (BMD) (z-score < -1) at baseline. The administration of Nutropin (n = 16) (0.025 mg/kg/day) for two years resulted in increased spine BMD from baseline when compared to placebo (n = 13) (4.6% vs. 1.0%, respectively, p<0.03); a transient decrease in spine BMD was seen at six months in the Nutropin-treated patients. Thirty-five percent of subjects treated with this dose had supraphysiological levels of IGF-I at some point during the study, which may carry unknown risks. No significant improvement in total body BMD was found when compared to placebo. A lower GH dose (0.0125 mg/kg/day) did not show significant increments in either of these bone parameters when compared to placebo. No statistically significant effects on BMD were seen in the adult-onset study where patients received GH (0.0125 mg/kg/day) for one year.
Muscle strength, physical endurance, and quality of life measurements were not markedly abnormal at baseline, and no statistically significant effects of Nutropin therapy were observed in the two studies.
INDICATIONS AND USAGE
Pediatric Patients
Nutropin AQ ® [somatropin (rDNA origin) injection] is indicated for the long-term treatment of growth failure due to a lack of adequate endogenous GH secretion.
Nutropin AQ ® [somatropin (rDNA origin) injection] is also indicated for the treatment of growth failure associated with chronic renal insufficiency up to the time of renal transplantation. Nutropin AQ therapy should be used in conjunction with optimal management of chronic renal insufficiency.
Nutropin AQ ® [somatropin (rDNA origin) injection] is also indicated for the long-term treatment of short stature associated with Turner syndrome.
Adult Patients
Nutropin AQ ® [somatropin (rDNA origin) injection] is indicated for the replacement of endogenous GH in patients with adult GH deficiency who meet both of the following two criteria:
- Biochemical diagnosis of adult GH deficiency by means of a subnormal response to a standard growth hormone stimulation test (peak GH </=5 µg/L), and
-
Adult-onset: Patients who have adult GH deficiency either alone or with multiple hormone deficiencies (hypopituitarism) as a result of pituitary disease, hypothalamic disease, surgery, radiation therapy, or trauma; or
Childhood-onset: Patients who were GH deficient during childhood, confirmed as an adult before replacement therapy with Nutropin AQ is started.
CONTRAINDICATIONS
Growth hormone should not be initiated to treat patients with acute critical illness due to complications following open heart or abdominal surgery, multiple accidental trauma or to patients having acute respiratory failure. Two placebo-controlled clinical trials in non-growth hormone-deficient adult patients (n = 522) with these conditions revealed a significant increase in mortality (41.9% vs. 19.3%) among somatropin-treated patients (doses 5.3-8 mg/day) compared to those receiving placebo (see WARNINGS ).
Nutropin AQ should not be used for growth promotion in pediatric patients with closed epiphyses.
Nutropin AQ should not be used in patients with active neoplasia. GH therapy should be discontinued if evidence of neoplasia develops.
Growth hormone is contraindicated in patients with Prader-Willi syndrome who are severely obese or have severe respiratory impairment (see WARNINGS ). Unless patients with Prader-Willi syndrome also have a diagnosis of growth hormone deficiency, Nutropin AQ is not indicated for the long-term treatment of pediatric patients who have growth failure due to genetically confirmed Parader-Willi syndrome.
WARNINGS
See CONTRAINDICATIONS for information on increased mortality in patients with acute critical illnesses in intensive care units due to complications following open heart or abdominal surgery, multiple accidental trauma, or with acute respiratory failure. The safety of continuing growth hormone treatment in patients receiving replacement doses for approved indications who concurrently develop these illnesses has not been established. Therefore, the potential benefit of treatment continuation with growth hormone in patients having acute critical illnesses should be weighed against the potential risk.
There have been reports of fatalities after initiating therapy with growth hormone in pediatric patients with Prader-Willi syndrome who had one or more of the following risk factors: severe obesity, history of upper airway obstruction or sleep apnea, or unidentified respiratory infection. Male patients with one or more of these factors may be at greater risk than females. Patients with Prader-Willi syndrome should be evaluated for signs of upper airway obstruction and sleep apnea before initiation of treatment with growth hormone. If, during treatment with growth hormone, patients show signs of upper airway obstruction (including onset of or increased snoring) and/or new onset sleep apnea, treatment should be interrupted. All patients with Prader-Willi syndrome treated with growth hormone should also have effective weight control and be monitored for signs of respiratory infection, which should be diagnosed as early as possible and treated aggressively (see CONTRAINDICATIONS ). Unless patients with Prader-Willi syndrome also have a diagnosis of growth hormone deficiency, Nutropin AQ is not indicated for the long-term treatment of pediatric patients who have growth failure due to genetically confirmed Parader-Willi syndrome.
PRECAUTIONS
General: Nutropin AQ should be prescribed by physicians experienced in the diagnosis and management of patients with GH deficiency, Turner syndrome, or chronic renal insufficiency (CRI). No studies have been completed of Nutropin AQ therapy in patients who have received renal transplants. Currently, treatment of patients with functioning renal allografts is not indicated.
Experience with prolonged rhGH treatment in adults is limited.
Geriatric Usage: Clinical studies of Nutropin AQ did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
Patients with epiphyseal closure who were treated with GH-replacement therapy in childhood should be re-evaluated according to the criteria in the INDICATIONS AND USAGE section before continuation of GH therapy at the reduced dose level recommended for GH-deficient adults.
Because Nutropin AQ may reduce insulin sensitivity, patients should be monitored for evidence of glucose intolerance.
For patients with diabetes mellitus, the insulin dose may require adjustment when GH therapy is instituted. Because GH may reduce insulin sensitivity, particularly in obese individuals, patients should be observed for evidence of glucose intolerance. Patients with diabetes or glucose intolerance should be monitored closely during GH therapy.
Nutropin therapy in adults with GH deficiency of adult onset was associated with an increase of median fasting insulin in the Nutropin 0.0125 mg/kg/day group from 9.0 µU/mL at baseline to 13.0 µU/mL at Month 12 with a return to the baseline median after a 3-week post-washout period off GH therapy. In the placebo group there was no change from 8.0 µU/mL at baseline to Month 12, and after the post-washout the median was 9.0 µU/mL. The between-treatment-groups difference in change from baseline to Month 12 was significant, p<0.0001. In childhood-onset subjects, there was a change of median fasting insulin in the Nutropin 0.025 mg/kg/day group from 11.0 µU/mL at baseline to 20.0 µU/mL at Month 12, in the Nutropin 0.0125 mg/kg/day group from 8.5 µU/mL to 11.0 µU/mL, and in the placebo group from 7.0 µU/mL to 8.0 µU/mL. The between-treatment-groups difference for these changes was significant, p = 0.0007.
In subjects with adult-onset GH deficiency, there was no between-treatment-group difference in changes from baseline to Month 12 in mean HbA 1c , p = 0.08. In childhood-onset mean HbA 1c increased in the Nutropin 0.025 mg/kg/day group from 5.2% at baseline to 5.5% at Month 12, and did not change in the Nutropin 0.0125 mg/kg/day group from 5.1% at baseline or in the placebo group from 5.3% at baseline. The between-treatment-groups difference was significant, p = 0.009.
Patients with a history of an intracranial lesion should be examined frequently for progression or recurrence of the lesion. In pediatric patients, clinical literature has demonstrated no relationship between GH-replacement therapy and central nervous system (CNS) tumor recurrence or new extracranial tumors. In adults, it is unknown whether there is any relationship between GH-replacement therapy and CNS tumor recurrence.
Patients with growth failure secondary to CRI should be examined periodically for evidence of progression of renal osteodystrophy. Slipped capital femoral epiphysis or avascular necrosis of the femoral head may be seen in children with advanced renal osteodystrophy, and it is uncertain whether these problems are affected by GH therapy. X-rays of the hip should be obtained prior to initiating GH therapy for CRI patients. Physicians and parents should be alert to the development of a limp or complaints of hip or knee pain in patients treated with Nutropin AQ.
Slipped capital femoral epiphysis may occur more frequently in patients with endocrine disorders or in patients undergoing rapid growth.
Progression of scoliosis can occur in patients who experience rapid growth. Because GH increases growth rate, patients with a history of scoliosis who are treated with GH should be monitored for progression of scoliosis. GH has not been shown to increase the incidence of scoliosis. Skeletal abnormalities including scoliosis are commonly seen in untreated Turner syndrome patients. Physicians should be alert to these abnormalities, which may manifest during GH therapy.
Patients with Turner syndrome should be evaluated carefully for otitis media and other ear disorders since these patients have an increased risk of ear or hearing disorders. In a randomized, controlled trial, there was a statistically significant increase, as compared to untreated controls, in otitis media (43% vs. 26%) and ear disorders (18% vs. 5%) in patients receiving GH. In addition, patients with Turner syndrome should be monitored closely for cardiovascular disorders (e.g., stroke, aortic aneurysm, hypertension) as these patients are also at risk for these conditions.
Intracranial hypertension (IH) with papilledema, visual changes, headache, nausea, and/or vomiting has been reported in a small number of patients treated with GH products. Symptoms usually occurred within the first eight (8) weeks of the initiation of GH therapy. In all reported cases, IH-associated signs and symptoms resolved after termination of therapy or a reduction of the GH dose. Funduscopic examination of patients is recommended at the initiation and periodically during the course of GH therapy. Patients with CRI and Turner syndrome may be at increased risk for development of IH.
As with any protein, local or systemic allergic reactions may occur. Parents/Patients should be informed that such reactions are possible and that prompt medical attention should be sought if allergic reactions occur.
Laboratory Tests: Serum levels of inorganic phosphorus, alkaline phosphatase, and parathyroid hormone (PTH) may increase with Nutropin AQ therapy.
Untreated hypothyroidism prevents optimal response to Nutropin AQ. Patients with Turner syndrome have an inherently increased risk of developing autoimmune thyroid disease. Changes in thyroid hormone laboratory measurements may develop during Nutropin AQ treatment. Therefore, patients should have periodic thyroid function tests and should be treated with thyroid hormone when indicated.
Drug Interactions: Excessive glucocorticoid therapy will inhibit the growth-promoting effect of human GH. Patients with ACTH deficiency should have their glucocorticoid-replacement dose carefully adjusted to avoid an inhibitory effect on growth.
The use of Nutropin AQ in patients with CRI receiving glucocorticoid therapy has not been evaluated. Concomitant glucocorticoid therapy may inhibit the growth-promoting effect of Nutropin AQ. If glucocorticoid replacement is required, the glucocorticoid dose should be carefully adjusted.
There was no evidence in the controlled studies of GH's interaction with drugs commonly used in chronic renal insufficiency patients. Limited published data indicate that GH treatment increases cytochrome P450 (CP450) mediated antipyrine clearance in man. These data suggest that GH administration may alter the clearance of compounds known to be metabolized by CP450 liver enzymes (e.g., corticosteroids, sex steroids, anticonvulsants, cyclosporin). Careful monitoring is advisable when GH is administered in combination with other drugs known to be metabolized by CP450 liver enzymes.
Carcinogenesis, Mutagenesis, Impairment of Fertility: Carcinogenicity, mutagenicity, and reproduction studies have not been conducted with Nutropin AQ.
Pregnancy: Pregnancy (Category C). Animal reproduction studies have not been conducted with Nutropin AQ. It is also not known whether Nutropin AQ can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. Nutropin AQ should be given to a pregnant woman only if clearly needed.
Nursing Mothers: It is not known whether Nutropin AQ is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when Nutropin AQ is administered to a nursing mother.
Information for Patients: Patients being treated with GH and/or their parents should be informed of the potential benefits and risks associated with treatment. If home use is determined to be desirable by the physician, instructions on appropriate use should be given, including a review of the contents of the Patient Information Insert. This information is intended to aid in the safe and effective administration of the medication. It is not a disclosure of all possible adverse or intended effects.
If home use is prescribed, a puncture-resistant container for the disposal of used syringes and needles should be recommended to the patient. Patients and/or parents should be thoroughly instructed in the importance of proper disposal and cautioned against any reuse of needles and syringes (see Patient Information Insert).
ADVERSE REACTIONS
As with all protein pharmaceuticals, a small percentage of patients may develop antibodies to the protein. GH antibody binding capacities below 2 mg/L have not been associated with growth attenuation. In some cases when binding capacity exceeds 2 mg/L, growth attenuation has been observed. In clinical studies of pediatric patients that were treated with Nutropin ® [somatropin (rDNA origin) for injection] for the first time, 0/107 growth hormone-deficient (GHD) patients, 0/125 CRI patients, and 0/112 Turner syndrome patients screened for antibody production developed antibodies with binding capacities >/=2 mg/L at six months. In a clinical study of patients that were treated with Nutropin AQ for the first time, 0/38 GHD patients screened for antibody production for up to 15 months developed antibodies with binding capacities >/=2 mg/L.
Additional short-term immunologic and renal function studies were carried out in a group of CRI patients after approximately one year of treatment to detect other potential adverse effects of antibodies to GH. Testing included measurements of C1q, C3, C4, rheumatoid factor, creatinine, creatinine clearance, and BUN. No adverse effects of GH antibodies were noted.
In addition to an evaluation of compliance with the prescribed treatment program and thyroid status, testing for antibodies to GH should be carried out in any patient who fails to respond to therapy.
Injection site discomfort has been reported. This is more commonly observed in children switched from another GH product to Nutropin AQ. Experience with Nutropin AQ in adults is limited.
Leukemia has been reported in a small number of GHD patients treated with GH. It is uncertain whether this increased risk is related to the pathology of GH deficiency itself, GH therapy, or other associated treatments such as radiation therapy for intracranial tumors. On the basis of current evidence, experts cannot conclude that GH therapy is responsible for these occurrences. The risk to GHD, CRI, or Turner syndrome patients, if any, remains to be established.
Other adverse drug reactions that have been reported in GH-treated patients include the following: 1) Metabolic: mild, transient peripheral edema. In GHD adults, edema or peripheral edema was reported in 41% of GH-treated patients and 25% of placebo-treated patients; 2) Musculoskeletal: arthralgias; carpal tunnel syndrome. In GHD adults, arthralgias and other joint disorders were reported in 27% of GH-treated patients and 15% of placebo-treated patients; 3) Skin: rare increased growth of pre-existing nevi; patients should be monitored for malignant transformation; and 4) Endocrine: gynecomastia. Rare pancreatitis.
OVERDOSAGE
Acute overdosage could lead to hyperglycemia. Long-term overdosage could result in signs and symptoms of gigantism and/or acromegaly consistent with the known effects of excess GH. (See recommended and maximal dosage instructions given below).
DOSAGE AND ADMINISTRATION
The Nutropin AQ dosage and administration schedule should be individualized for each patient. Response to GH therapy in pediatric patients tends to decrease with time. However, in pediatric patients whose failure to increase growth rate, particularly during the first year of therapy, suggests the need for close assessment of compliance and evaluation of other causes of growth failure, such as hypothyroidism, under-nutrition, and advanced bone age.
Dosage
Pediatric Growth Hormone Deficiency (GHD)
A weekly dosage of up to 0.3 mg/kg of body weight divided into daily subcutaneous injection is recommended. In pubertal patients, a weekly dosage of up to 0.7 mg/kg divided daily may be used.
Adult Growth Hormone Deficiency (GHD)
The recommended dosage at the start of therapy is not more than 0.006 mg/kg given as a daily subcutaneous injection. The dose may be increased according to individual patient requirements to a maximum of 0.025 mg/kg daily in patients under 35 years and to a maximum of 0.0125 mg/kg daily in patients over 35 years.
To minimize the occurrence of adverse events in older or overweight patients, lower doses may be necessary. During therapy, dosage should be decreased if required by the occurrence of side effects or excessive IGF-I levels.
Chronic Renal Insufficiency (CRI)
A weekly dosage of up to 0.35 mg/kg of body weight divided into daily subcutaneous injection is recommended.
Nutropin AQ therapy may be continued up to the time of renal transplantation.
In order to optimize therapy for patients who require dialysis, the following guidelines for injection schedule are recommended:
- Hemodialysis patients should receive their injection at night just prior to going to sleep or at least 3-4 hours after their hemodialysis to prevent hematoma formation due to the heparin.
- Chronic Cycling Peritoneal Dialysis (CCPD) patients should receive their injection in the morning after they have completed dialysis.
- Chronic Ambulatory Peritoneal Dialysis (CAPD) patients should receive their injection in the evening at the time of the overnight exchange.
Turner Syndrome
A weekly dosage of up to 0.375 mg/kg of body weight divided into equal doses 3 to 7 times per week by subcutaneous injection is recommended.
Administration
The solution should be clear immediately after removal from the refrigerator. Occasionally, after refrigeration, you may notice that small colorless particles of protein are present in the solution. This is not unusual for solutions containing proteins. Allow the vial or pen cartridge to come to room temperature and gently swirl. If the solution is cloudy, the contents MUST NOT be injected.
For Nutropin AQ ® Vial
Before needle insertion, wipe the septum of the Nutropin AQ vial with rubbing alcohol or an antiseptic solution to prevent contamination of the contents by microorganisms that may be introduced by repeated needle insertions. It is recommended that Nutropin AQ be administered using sterile, disposable syringes and needles. The syringes should be of small enough volume that the prescribed dose can be drawn from the vial with reasonable accuracy.
For Nutropin AQ Pen ® Cartridge
The Nutropin AQ pen cartridge is intended for use only with the Nutropin AQ Pen ® . Wipe the septum of the Nutropin AQ pen cartridge with rubbing alcohol or an antiseptic solution to prevent contamination of the contents by microorganisms that may be introduced by repeated needle insertions. It is recommended that Nutropin AQ be administered using sterile, disposable needles. Follow the directions provided in the Nutropin AQ Pen ® Instructions for Use.
The Nutropin AQ pen allows for administration of a minimum dose of 0.1 mg to a maximum dose of 4.0 mg, in 0.1 mg increments.
STABILITY AND STORAGE
Vial and cartridge contents are stable for 28 days after initial use when stored at 2-8°C/36-46°F (under refrigeration). Avoid freezing the vial or the cartridge of Nutropin AQ. The vials and cartridges of Nutropin AQ are light sensitive and they should be protected from light. Store the vial and cartridge refrigerated in a dark place when they are not in use.
HOW SUPPLIED
Nutropin AQ is supplied as either 10 mg (approximately 30 International Units) of sterile liquid somatropin per vial, or as 10 mg (approximately 30 International Units) of sterile liquid somatropin per pen cartridge.
Each vial carton contains one single vial containing 2 mL of Nutropin AQ ® [somatropin (rDNA origin) injection] 10 mg/2 mL (5 mg/mL). NDC 50242-022-20.
Each pen cartridge carton contains one single pen cartridge containing 2 mL of Nutropin AQ ® [somatropin (rDNA origin) injection] 10 mg/2 mL (5 mg/mL). NDC 50242-043-14.
Nutropin AQ ®
[somatropin (rDNA origin) injection]
Manufactured by:
Genentech, Inc.
1 DNA Way(4814906)
South San Francisco, CA 94080-4990
FDA Approval Date April 2002
Code Revision Date April 2004
©2004 Genentech, Inc.
-
Tissue Growth
Subscribe to the "News" RSS Feed 
TOP ۞