-
Renagel Tablets (Genzyme)
DESCRIPTION
The active ingredient in Renagel * Tablets is sevelamer hydrochloride, a polymeric phosphate binder intended for oral administration. Sevelamer hydrochloride is poly(allylamine hydrochloride) crosslinked with epichlorohydrin in which forty percent of the amines are protonated. It is known chemically as poly(allylamine- co -N,N'-diallyl-1,3-diamino-2-hydroxypropane) hydrochloride. Sevelamer hydrochloride is hydrophilic, but insoluble in water. The structure is represented below:
Chemical Structure of Sevelamer Hydrochloride
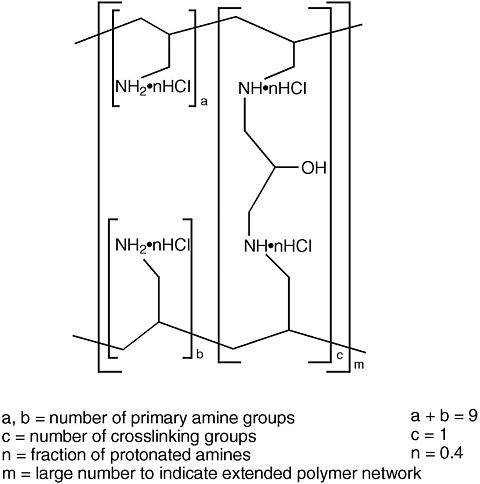
The primary amine groups shown in the structure are derived directly from poly(allylamine hydrochloride). The crosslinking groups consist of two secondary amine groups derived from poly(allylamine hydrochloride) and one molecule of epichlorohydrin.
Renagel® Tablets: Each film-coated tablet of Renagel contains either 800 mg or 400 mg of sevelamer hydrochloride on an anhydrous basis. The inactive ingredients are hypromellose, diacetylated monoglyceride, colloidal silicon dioxide, and stearic acid. The tablet imprint contains iron oxide black ink.
*Registered trademark of Genzyme Corporation.
CLINICAL PHARMACOLOGY
Patients with end-stage renal disease (ESRD) retain phosphorus and can develop hyperphosphatemia. High serum phosphorus can precipitate serum calcium resulting in ectopic calcification. When the product of serum calcium and phosphorus concentrations (Ca × P) exceeds 55 mg 2 /dL 2 , there is an increased risk that ectopic calcification will occur. Hyperphosphatemia plays a role in the development of secondary hyperparathyroidism in renal insufficiency. An increase in parathyroid hormone (PTH) levels is characteristic of patients with chronic renal failure. Increased levels of PTH can lead to osteitis fibrosa, a bone disease. A decrease in serum phosphorus may decrease serum PTH levels.
Treatment of hyperphosphatemia includes reduction in dietary intake of phosphate, inhibition of intestinal phosphate absorption with phosphate binders, and removal of phosphate with dialysis. Renagel taken with meals has been shown to decrease serum phosphorus concentrations in patients with ESRD who are on hemodialysis. In vitro studies have shown that the capsule and tablet formulations bind phosphate to a similar extent. Renagel does not contain aluminum or other metals and does not cause aluminumin toxication.
Renagel treatment also results in a lowering of low-density lipoprotein (LDL) and total serum cholesterol levels.
Pharmacokinetics: A mass balance study using 14 C-sevelamer hydrochloride in 16 healthy male and female volunteers showed that sevelamer hydrochloride is not systemically absorbed. No absorption studies have been performed in patients with renal disease.
Clinical trials: The ability of Renagel Capsules to lower serum phosphorus in ESRD patients on hemodialysis was demonstrated in six clinical trials: one double-blind placebo controlled 2-week study (renagel N=24); two open-label uncontrolled 8-week studies (renagel N=220) and three active-controlled open-label studies with treatment durations of 8 to 52 weeks (renagel N=256). Two of the active-controlled studies are described here. One trial is a crossover trial with two 8-week periods comparing Renagel to calcium acetate and the other trial is a 52-week parallel design trial comparing Renagel tablets with calcium acetate and calcium carbonate.
Cross-over study of Renagel Capsules and calcium acetate: Eighty-four ESRD patients on hemodialysis who were hyperphosphatemic (serum phosphorus > 6.0 mg/dL) following a two-week phosphate binder washout period were randomized to receive either Renagel Capsules for eight weeks followed by calcium acetate for eight weeks or calcium acetate for eight weeks followed by Renagel Capsules for eight weeks. Treatment periods were separated by a two-week phosphate binder washout period. Patients started on Renagel Capsules or calcium acetate tablets three times per day with meals. Over each eight-week treatment period, at three separate time points the dose of either agent could be titrated up 1 capsule or tablet per meal (3 per day) to control serum phosphorus. Renagel Capsules and calcium acetate both significantly decreased mean serum phosphorus by about 2 mg/dL (Table 1).
Table 1. Mean Serum Phosphorus (mg/dL) at Baseline and Endpoint Renagel
(N=81)Calcium
(N=83)Baseline at End of Washout8.4 8.0 Change from Baseline
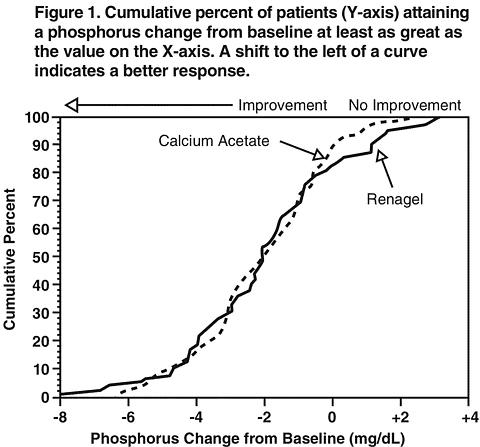
at Endpoint-2.0 * -2.1 * (95% Confidence Interval)(-2.5, -1.5) (-2.6, -1.7) *p <0.0001, within treatment group comparison Figure 1 illustrates that the proportion of patients achieving a given level of serum phosphorus lowering is comparable between the two treatment groups. For example, about half the patients in each group had a decrease of at least 2 mg/dL at endpoint.
Average daily consumption at the end of treatment was 4.9 g sevelamer hydrochloride (range of 0.0 to 12.6 g) and 5.0 g of calcium acetate (range of 0.0 to 17.8 g). During calcium acetate treatment, 22% of patients developed serum calcium >/= 11.0 mg/dL on at least one occasion versus 5% for Renagel (p < 0.05). Thus the risk of developing hypercalcemia is less with Renagel Capsules compared to calcium acetate.
Mean LDL cholesterol and mean total cholesterol declined significantly on Renagel Capsules treatment (-24% and -15%, respectively). Neither LDL nor total cholesterol changed on calcium acetate treatment. Triglycerides, high-density lipoprotein (HDL) cholesterol, and albumin did not change on either treatment.
Similar reductions in serum phosphorus and LDL cholesterol were observed in an eight-week open-label, uncontrolled study of 172 end stage renal disease patients on hemodialysis.
Parallel study of Renagel and calcium acetate or calcium carbonate: Two hundred ESRD patients on hemodialysis who were hyperphosphatemic (serum phosphorus >5.5 mg/dL) following a two-week phosphate binder washout period were randomized to receive Renagel 800 mg tablets (N=99) or calcium, either calcium acetate (N=54) or calcium carbonate (N=47). Calcium acetate and calcium carbonate produced comparable decreases in serum phosphorus. At week 52, using last-observation-carried-forward, Renagel and Calcium both significantly decreased mean serum phosphorus (Table 2).
Table 2. Mean Serum Phosphorus (mg/dL) and Ion Product at Baseline and End of Treatment Renagel
(N=94)Calcium
(N=98)Phosphorus
Baseline7.5 7.3 Change from Baseline at Endpoint-2.1 -1.8 Ca × Phosphorus Ion Product
Baseline70.5 68.4 Change from Baseline at Endpoint-19.4 -14.2 Sixty-one percent of Renagel patients and 73% of the calcium patients completed the full 52 weeks of treatment. The major reason for dropout in the Renagel group was gastrointestinal adverse events.
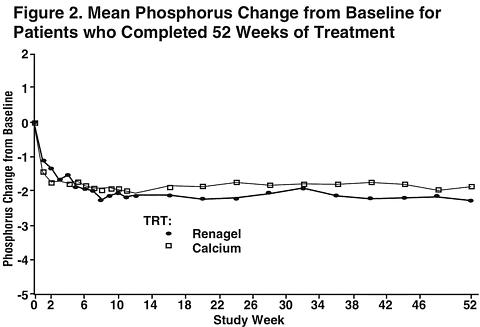
Figure 2, a plot of the phosphorus change from baseline for the completers, illustrates the durability of response for patients who are able to remain on treatment.
Average daily consumption at the end of treatment was 6.5 g of sevelamer hydrochloride (range of 0.8 to 13 g) or approximately eight 800 mg tablets (range of 1 to 16 tablets), 4.6 g of calcium acetate (range of 0.7 to 9.5 g) and 3.9 g of calcium carbonate (range 1.3 to 9.1 g). During calcium treatment, 34% of patients developed serum calcium corrected for albumin >/= 11.0 mg/dL on at least one occasion versus 7% for Renagel (p<0.05). Thus the risk of developing hypercalcemia is less with Renagel compared to calcium salts.
Mean LDL cholesterol and mean total cholesterol declined significantly (p<0.05) on Renagel treatment (-32% and -20%, respectively) compared to calcium (+0.2% and -2%, respectively). Triglycerides, HDL cholesterol, and albumin did not change.
INDICATIONS AND USAGE
Renagel is indicated for the control of serum phosphorus in patients with Chronic Kidney Disease (CKD) on hemodialysis. The safety and efficacy of Renagel in CKD patients who are not on hemodialysis have not been studied. In hemodialysis patients, Renagel decreases the incidence of hypercalcemic episodes relative to patients on calcium treatment.
CONTRAINDICATIONS
Renagel is contraindicated in patients with hypophosphatemia or bowel obstruction. Renagel is contraindicated in patients known to be hypersensitive to sevelamer hydrochloride or any of its constituents.
PRECAUTIONS
General: The safety and efficacy of Renagel in patients with dysphagia, swallowing disorders, severe gastrointestinal (GI) motility disorders, or major GI tract surgery have not been established. Consequently, caution should be exercised when Renagel is used in patients with these GI disorders.
Renagel does not contain calcium or alkali supplementation; serum calcium, bicarbonate, and chloride levels should be monitored.
In preclinical studies in rats and dogs, sevelamer hydrochloride reduced vitamin D, E, K, and folic acid levels at doses of 6-100 times the recommended human dose. In clinical trials, there was no evidence of reduction in serum levels of vitamins with the exception of a one year clinical trial in which Renagel treatment was associated with reduction of 25-hydroxyvitamin D (normal range 10 to 55 mcg/mL) from 39 ± 22 mcg/mL to 34 ± 22 mcg/mL (p<0.01). Most (approximately 75%) patients in Renagel clinical trials received vitamin supplements, which is typical of patients on hemodialysis.
Information for the patient: The prescriber should inform patients to take Renagel with meals and adhere to their prescribed diets. Instructions should be given on concomitant medications that should be dosed apart from Renagel. Because the contents of Renagel expand in water, tablets should be swallowed intact and should not be crushed, chewed, broken into pieces, or taken apart prior to administration.
Drug interactions: Renagel Capsules were studied in human drug-drug interaction studies with ciprofloxacin, digoxin, warfarin, enalapril, metoprolol and iron.
Ciprofloxacin: In a study of 15 healthy subjects, a co-administered single dose of 7 Renagel Capsules (approximately 2.8g) decreased the bioavailability of ciprofloxacin by approximately 50%.
Digoxin: In 19 healthy subjects receiving 6 Renagel capsules three times a day with meals for 2 days, Renagel did not alter the pharmacokinetics of a single dose of digoxin.
Warfarin: In 14 healthy subjects receiving 6 Renagel capsules three times a day with meals for 2 days, Renagel did not alter the pharmacokinetics of a single dose of warfarin.
Enalapril: In 28 healthy subjects a single dose of 6 Renagel capsules did not alter the pharmacokinetics of a single dose of enalapril.
Metoprolol: In 31 healthy subjects a single dose of 6 Renagel capsules did not alter the pharmacokinetics of a single dose of metoprolol.
Iron: In 23 healthy subjects, a single dose of 7 Renagel capsules did not alter the absorption of a single oral dose of iron as 200 mg exsiccated ferrous sulfate tablet.
Furthermore, when administering an oral medication where a reduction in the bioavailability of that medication would have a clinically significant effect on its safety or efficacy, the drug should be administered at least one hour before or three hours after Renagel, or the physician should consider monitoring blood levels of the drug. Patients taking anti-arrhythmic and anti-seizure medications were excluded from the clinical trials. Special precautions should be taken when prescribing Renagel to patients also taking these medications.
Carcinogenesis, mutagenesis, and impairment of fertility: Standard lifetime carcinogenicity bioassays were conducted in mice and rats. Rats were given sevelamer hydrochloride by diet at 0.3, 1, 3 g/kg/day. There was an increased incidence of urinary bladder transitional cell papilloma in male rats (3 g/kg/day) at exposures 2 times the maximum human oral dose of 13 g, based on a comparison of relative body surface area. Mice received mean dietary doses of 0.8, 3, 9 g/kg/day. Increased incidence of tumors was not observed in mice at exposures up to 3 times the maximum human oral dose of 13g, based on a comparison of relative body surface area.
In an in vitro mammalian cytogenetic test with metabolic activation, sevelamer hydrochloride caused a statistically significant increase in the number of structural chromosome aberrations. Sevelamer hydrochloride was not mutagenic in the Ames bacterial mutation assay.
In a study designed to assess potential impairment of fertility, female rats were given dietary doses of 0.5, 1.5, 4.5 g/kg/day beginning 14 days prior to mating and continuing through gestation. Male rats were given the same doses and treated for 28 days before mating. Sevelamer hydrochloride did not impair fertility in male or female rats at exposures 3 times the maximum human oral dose of 13 g, based on a comparison of relative body surface area.
Pregnancy:
Pregnancy Category C
In pregnant rats given dietary doses of 0.5, 1.5, 4.5 g/kg/day during organogenesis, reduced or irregular ossification of fetal bones, probably due to a reduced absorption of fat-soluble vitamin D occurred in the mid and high dose groups (exposures less than the maximum human dose of 13g, based on a comparison of relative body surface area). In pregnant rabbits given oral doses of 100, 500, 1000 mg/kg/day by gavage during organogenesis an increased incidence of early resorptions occurred at exposures 2 times the maximum human dose of 13 g, based on a comparison of relative body surface area. Requirements for vitamins and other nutrients are increased in pregnancy. The effect of Renagel on the absorption of vitamins and other nutrients has not been studied in pregnant women.
Geriatric use: There is no evidence for special considerations when Renagel is administered to elderly patients.
Pediatric use: The safety and efficacy of Renagel has not been established in pediatric patients.
ADVERSE REACTIONS
In a placebo-controlled study with a treatment duration of two weeks, the adverse events reported for Renagel Capsules (N=24) were similar to those reported for placebo (N=12). In a cross-over study with treatment durations of eight weeks each, the adverse events reported for Renagel Capsules (N=82) were similar to those reported for calcium acetate (N=82) and included headache, infection, pain, hypertension, hypotension, thrombosis, diarrhea, dyspepsia, vomiting, and cough increased. In a parallel design study with treatment duration of 52 weeks, adverse events reported for Renagel Tablets (N=99) were similar to those reported for calcium (calcium acetate and calcium carbonate) (N=101). (Table 3).
Table 3. Treatment-Emergent Adverse Events >/= 10 % from a Parallel Design Trial of Renagel Tablets versus Calcium for 52 Weeks of Treatment Adverse EventRenagel
(N=99)Calcium
(N=101)Patients
%Patients
%Gastrointestinal DisordersVomiting22.2 21.8 Nausea20.2 19.8 Diarrhea19.2 22.8 Dyspepsia16.2 6.9 Constipation8.1 11.9 Infections and InfestationsNasopharyngitis14.1 7.9 Bronchitis11.1 12.9 Upper Respiratory Tract Infection5.1 10.9 Musculoskeletal, Connective Tissue and Bone DisordersPain in Limb13.1 14.9 Arthralgia12.1 17.8 Back Pain4.0 17.8 Skin DisordersPruritus13.1 9.9 Respiratory, Thoracic and Mediastinal DisordersDyspnea10.1 16.8 Cough7.1 12.9 Vascular DisordersHypertension10.1 5.9 Nervous System DisordersHeadache9.1 15.8 General Disorders and Site Administration DisordersMechanical Complication of Implant6.1 10.9 Pyrexia5.1 10.9 In the parallel design study, the major reason for drop out in the Renagel group was gastrointestinal adverse events. In a long-term, open-label extension trial, adverse events possibly related to Renagel Capsules and which were not dose-related, included nausea (7%), constipation (2%), diarrhea (4%), flatulence (4%), and dyspepsia (5%). During post-marketing experience, the following adverse events have been reported in patients receiving Renagel although no direct relationship to Renagel could be established: pruritis, rash, and abdominal pain.
OVERDOSAGE
Renagel has been given to normal healthy volunteers in doses of up to 14 grams per day for eight days with no adverse effects. Renagel has been given in average doses up to 13 grams per day to hemodialysis patients. There are no reported overdosages of Renagel in patients. Since Renagel is not absorbed, the risk of systemic toxicity is low.
DOSAGE AND ADMINISTRATION
Patients Not Taking a Phosphate Binder. The recommended starting dose of Renagel is 800 to 1600 mg, which can be administered as one to two Renagel® 800 mg Tablets or two to four Renagel® 400 mg Tablets with each meal based on serum phosphorus level. Table 4 provides recommended starting doses of Renagel for patients not taking a phosphate binder.
Table 4. Starting Dose for Patients Not Taking a Phosphate Binder SERUM
PHOSPHORUSRENAGEL®
800 MGRENAGEL®
400 MG> 5.5 and
< 7.5 mg/dL1 tablet
three times daily
with meals2 tablets
three times daily
with meals>/= 7.5 and
< 9.0 mg/dL2 tablets
three times daily
with meals3 tablets
three times daily
with meals>/= 9.0 mg/dL 2 tablets
three times daily
with meals4 tablets
three times daily
with mealsPatients Switching From Calcium Acetate. In a study in 84 ESRD patients on hemodialysis, a similar reduction in serum phosphorus was seen with equivalent doses (mg for mg) of Renagel Capsules and calcium acetate. Table 5 gives recommended starting doses of Renagel based on a patient's current calcium acetate dose.
Table 5. Starting Dose for Patients Switching From Calcium Acetate to Renagel CALCIUM
ACETATE 667 MG
(TABLETS
PER MEAL)RENAGEL®
800 MG
(TABLETS
PER MEAL)RENAGEL®
400 MG
(TABLETS
PER MEAL)1 tablet 1 tablet 2 tablets 2 tablets 2 tablets 3 tablets 3 tablets 3 tablets 5 tablets Dose Titration for All Patients Taking Renagel. Dosage should be adjusted based on the serum phosphorus concentration with a goal of lowering serum phosphorus to 5.5 mg/dL or less. The dose may be increased or decreased by one tablet per meal at two week intervals as necessary. Table 6 gives a dose titration guideline. The average dose in a Phase 3 trial designed to lower serum phosphorus to 5.0 mg/dL or less was approximately three Renagel 800 mg tablets per meal. The maximum average daily Renagel dose studied was 13 grams.
Table 6. Dose Titration Guideline SERUM PHOSPHORUSRENAGEL
DOSE> 5.5 mg/dLIncrease 1 tablet per meal at 2 week intervals3.5-5.5 mg/dLMaintain current dose< 3.5 mg/dLDecrease 1 tablet per mealDrug interaction studies have demonstrated that Renagel Capsules have no effect on the bioavailability of digoxin, warfarin, enalapril, metoprolol, or iron. However, the bioavailability of ciprofloxacin was decreased by approximately 50% when co-administered with Renagel or calcium acetate, in a single dose study. When administering an oral drug for which alteration in blood levels could have a clinically significant effect on its safety or efficacy, the drug should be administered at least one hour before or three hours after Renagel, or the physician should consider monitoring blood levels of the drug. (See PRECAUTIONS : Drug interactions .)
Do not use Renagel after the expiration date on the bottle.
HOW SUPPLIED
Renagel® 800 mg Tablets are supplied as oval, film-coated, compressed tablets, imprinted with "RENAGEL 800," containing 800 mg of sevelamer hydrochloride on an anhydrous basis, hypromellose, diacetylated monoglyceride, colloidal silicon dioxide, and stearic acid. Renagel® 800 mg Tablets are packaged in bottles of 180 tablets.
NDC 58468-0021-1 Bottle of 180 Tablets
Renagel® 400 mg Tablets are supplied as oval, film-coated, compressed tablets, imprinted with "RENAGEL 400," containing 400 mg of sevelamer hydrochloride on an anhydrous basis, hypromellose, diacetylated monoglyceride, colloidal silicon dioxide, and stearic acid. Renagel® 400 mg Tablets are packaged in bottles of 360 tablets.
NDC 58468-0020-1 Bottle of 360 Tablets
Storage
Store at 25°C (77°F): excursions permitted to 15-30°C (59-86°F).
[See USP controlled room temperature]
Protect from moisture.
Rx only
Distributed by:
Genzyme Corporation
500 Kendall Street
Cambridge, MA 02142
USA
Tel. (800) 847-0069
4777
102604R02
Issued 10/04
Subscribe to the "News" RSS Feed 
TOP ۞