-
Viramune Oral Suspension, Viramune Tablets (Boehringer Ingelheim)
WARNING
Severe, life-threatening, and in some cases fatal hepatotoxicity, particularly in the first 18 weeks, has been reported in patients treated with VIRAMUNE®. In some cases, patients presented with non-specific prodromal signs or symptoms of hepatitis and progressed to hepatic failure. These events are often associated with rash. Female gender and higher CD4 counts at initiation of therapy place patients at increased risk; women with CD4 counts >250 cells/mm 3 , including pregnant women receiving VIRAMUNE in combination with other antiretrovirals for the treatment of HIV infection, are at the greatest risk. However, hepatotoxicity associated with VIRAMUNE use can occur in both genders, all CD4 counts and at any time during treatment. Patients with signs or symptoms of hepatitis, or with increased transaminases combined with rash or other systemic symptoms, must discontinue VIRAMUNE and seek medical evaluation immediately (see WARNINGS ).
Severe, life-threatening skin reactions, including fatal cases, have occurred in patients treated with VIRAMUNE. These have included cases of Stevens-Johnson syndrome, toxic epidermal necrolysis, and hypersensitivity reactions characterized by rash, constitutional findings, and organ dysfunction. Patients developing signs or symptoms of severe skin reactions or hypersensitivity reactions must discontinue VIRAMUNE and seek medical evaluation immediately (see WARNINGS ).
It is essential that patients be monitored intensively during the first 18 weeks of therapy with VIRAMUNE to detect potentially life-threatening hepatotoxicity or skin reactions. Extra vigilance is warranted during the first 6 weeks of therapy, which is the period of greatest risk of these events. Do not restart VIRAMUNE following severe hepatic, skin or hypersensitivity reactions. In some cases, hepatic injury has progressed despite discontinuation of treatment. In addition, the 14-day lead-in period with VIRAMUNE 200 mg daily dosing must be strictly followed (see WARNINGS ).
DESCRIPTION
VIRAMUNE is the brand name for nevirapine (NVP), a non-nucleoside reverse transcriptase inhibitor with activity against Human Immunodeficiency Virus Type 1 (HIV-1). Nevirapine is structurally a member of the dipyridodiazepinone chemical class of compounds.
VIRAMUNE Tablets are for oral administration. Each tablet contains 200 mg of nevirapine and the inactive ingredients microcrystalline cellulose, lactose monohydrate, povidone, sodium starch glycolate, colloidal silicon dioxide and magnesium stearate.
VIRAMUNE Oral Suspension is for oral administration. Each 5 mL of VIRAMUNE suspension contains 50 mg of nevirapine (as nevirapine hemihydrate). The suspension also contains the following excipients: carbomer 934P, methylparaben, propylparaben, sorbitol, sucrose, polysorbate 80, sodium hydroxide and purified water.
The chemical name of nevirapine is 11-cyclopropyl-5,11-dihydro-4-methyl-6H-dipyrido [3,2-b:2',3'-e][1,4] diazepin-6-one. Nevirapine is a white to off-white crystalline powder with the molecular weight of 266.30 and the molecular formula C 15 H 14 N 4 O. Nevirapine has the following structural formula:
MICROBIOLOGY
Mechanism of Action:
Nevirapine is a non-nucleoside reverse transcriptase inhibitor (NNRTI) of HIV-1. Nevirapine binds directly to reverse transcriptase (RT) and blocks the RNA-dependent and DNA-dependent DNA polymerase activities by causing a disruption of the enzyme's catalytic site. The activity of nevirapine does not compete with template or nucleoside triphosphates. HIV-2 RT and eukaryotic DNA polymerases (such as human DNA polymerases (alpha), (beta), (gamma), or [dgr ]) are not inhibited by nevirapine.
Antiviral Activity:
The in vitro antiviral activity of nevirapine was measured in peripheral blood mononuclear cells, monocyte derived macrophages, and lymphoblastoid cell lines. IC 50 values (50% inhibitory concentration) ranged from 10-100 nM against laboratory and clinical isolates of HIV-1. In cell culture, nevirapine demonstrated additive to synergistic activity against HIV-1 in drug combination regimens with the nucleoside reverse transcriptase inhibitors (NRTIs) didanosine (ddI), lamivudine (3TC), stavudine (d4T) and zidovudine (ZDV), and the protease inhibitors indinavir and saquinavir.
Resistance:
HIV-1 isolates with reduced susceptibility (100-250-fold) to nevirapine emerge in vitro . Genotypic analysis showed mutations in the HIV-1 RT gene Y181C and/or V106A depending upon the virus strain and cell line employed. Time to emergence of nevirapine resistance in vitro was not altered when selection included nevirapine in combination with several other NNRTIs.
Phenotypic and genotypic changes in HIV-1 isolates from treatment-na[iuml ]ve patients receiving either nevirapine (n=24) or nevirapine and ZDV (n=14) were monitored in Phase I/II trials over 1 to >/=12 weeks. After 1 week of nevirapine monotherapy, isolates from 3/3 patients had decreased susceptibility to nevirapine in vitro . One or more of the RT mutations resulting in amino acid substitutions K103N, V106A, V108I, Y181C, Y188C and G190A were detected in HIV-1 isolates from some patients as early as 2 weeks after therapy initiation. By week eight of nevirapine monotherapy, 100% of the patients tested (n=24) had HIV-1 isolates with a >100-fold decrease in susceptibility to nevirapine in vitro compared to baseline, and had one or more of the nevirapine-associated RT resistance mutations. Nineteen of these patients (80%) had isolates with Y181C mutations regardless of dose.
Genotypic analysis of isolates from antiretroviral na[iuml ]ve virologic failure patients (n=71) receiving nevirapine once daily (n=25) or twice daily (n=46) in combination with lamivudine and stavudine (study 2NN) for 48 weeks showed that isolates from 8/25 and 23/46 patients, respectively, contained one or more of the following NNRTI resistance-associated mutations: Y181C, K101E, G190A/S, K103N, V106A/M, V108I, Y188C/L, A98G, F227L and M230L.
Cross-resistance:
Rapid emergence of HIV-1 strains which are cross-resistant to NNRTIs has been observed in vitro . Nevirapine-resistant HIV-1 isolates were cross-resistant to the NNRTIs delavirdine and efavirenz. However, nevirapine-resistant isolates were susceptible to the NNRTI's ddI and ZDV. Similarly, ZDV-resistant isolates were susceptible to nevirapine in vitro .
ANIMAL PHARMACOLOGY
Animal studies have shown that nevirapine is widely distributed to nearly all tissues and readily crosses the blood-brain barrier.
CLINICAL PHARMACOLOGY
Pharmacokinetics in Adults:
Absorption and Bioavailability: Nevirapine is readily absorbed (>90%) after oral administration in healthy volunteers and in adults with HIV-1 infection. Absolute bioavailability in 12 healthy adults following single-dose administration was 93 ± 9% (mean ± SD) for a 50 mg tablet and 91 ± 8% for an oral solution. Peak plasma nevirapine concentrations of 2 ± 0.4 µg/mL (7.5 µM) were attained by 4 hours following a single 200 mg dose. Following multiple doses, nevirapine peak concentrations appear to increase linearly in the dose range of 200 to 400 mg/day. Steady state trough nevirapine concentrations of 4.5 ± 1.9 µg/mL (17 ± 7 µM), (n = 242) were attained at 400 mg/day. Nevirapine tablets and suspension have been shown to be comparably bioavailable and interchangeable at doses up to 200 mg. When VIRAMUNE (200 mg) was administered to 24 healthy adults (12 female, 12 male), with either a high fat breakfast (857 kcal, 50 g fat, 53% of calories from fat) or antacid (Maalox® 30 mL), the extent of nevirapine absorption (AUC) was comparable to that observed under fasting conditions. In a separate study in HIV-1 infected patients (n=6), nevirapine steady-state systemic exposure (AUC[tgr ]) was not significantly altered by didanosine, which is formulated with an alkaline buffering agent. VIRAMUNE may be administered with or without food, antacid or didanosine.
Distribution: Nevirapine is highly lipophilic and is essentially nonionized at physiologic pH. Following intravenous administration to healthy adults, the apparent volume of distribution (Vdss) of nevirapine was 1.21 ± 0.09 L/kg, suggesting that nevirapine is widely distributed in humans. Nevirapine readily crosses the placenta and is also found in breast milk (see PRECAUTIONS , Nursing Mothers ). Nevirapine is about 60% bound to plasma proteins in the plasma concentration range of 1-10 µg/mL. Nevirapine concentrations in human cerebrospinal fluid (n=6) were 45% (± 5%) of the concentrations in plasma; this ratio is approximately equal to the fraction not bound to plasma protein.
Metabolism/Elimination: In vivo studies in humans and in vitro studies with human liver microsomes have shown that nevirapine is extensively biotransformed via cytochrome P450 (oxidative) metabolism to several hydroxylated metabolites. In vitro studies with human liver microsomes suggest that oxidative metabolism of nevirapine is mediated primarily by cytochrome P450 (CYP) isozymes from the CYP3A4 and CYP2B6 families, although other isozymes may have a secondary role. In a mass balance/excretion study in eight healthy male volunteers dosed to steady state with nevirapine 200 mg given twice daily followed by a single 50 mg dose of 14 C-nevirapine, approximately 91.4 ± 10.5% of the radiolabeled dose was recovered, with urine (81.3 ± 11.1%) representing the primary route of excretion compared to feces (10.1 ± 1.5%). Greater than 80% of the radioactivity in urine was made up of glucuronide conjugates of hydroxylated metabolites. Thus cytochrome P450 metabolism, glucuronide conjugation, and urinary excretion of glucuronidated metabolites represent the primary route of nevirapine biotransformation and elimination in humans. Only a small fraction (<5%) of the radioactivity in urine (representing <3% of the total dose) was made up of parent compound; therefore, renal excretion plays a minor role in elimination of the parent compound.
Nevirapine is an inducer of hepatic cytochrome P450 (CYP) metabolic enzymes 3A4 and 2B6. Nevirapine induces CYP3A4 and CYP2B6 by approximately 20-25%, as indicated by erythromycin breath test results and urine metabolites. Autoinduction of CYP3A4 and CYP2B6 mediated metabolism leads to an approximately 1.5 to 2 fold increase in the apparent oral clearance of nevirapine as treatment continues from a single dose to two-to-four weeks of dosing with 200-400 mg/day. Autoinduction also results in a corresponding decrease in the terminal phase half-life of nevirapine in plasma, from approximately 45 hours (single dose) to approximately 25-30 hours following multiple dosing with 200-400 mg/day.
Pharmacokinetics in Special Populations:
Renal Impairment: HIV seronegative adults with mild (CrCL 50-79 mL/min; n=7), moderate (CrCL 30-49 mL/min; n=6), or severe (CrCL <30 mL/min; n=4) renal impairment received a single 200 mg dose of nevirapine in a pharmacokinetic study. These subjects did not require dialysis. The study included six additional subjects with renal failure requiring dialysis.
In subjects with renal impairment (mild, moderate or severe), there were no significant changes in the pharmacokinetics of nevirapine. However, subjects requiring dialysis exhibited a 44% reduction in nevirapine AUC over a one-week exposure period. There was also evidence of accumulation of nevirapine hydroxy-metabolites in plasma in subjects requiring dialysis. An additional 200 mg dose following each dialysis treatment is indicated (see DOSAGE AND ADMINISTRATION ; PRECAUTIONS ).
Hepatic Impairment: HIV seronegative adults with mild (Child-Pugh Class A; n=6) or moderate (Child-Pugh Class B; n=4) hepatic impairment received a single 200 mg dose of nevirapine in a pharmacokinetic study.
In the majority of patients with mild or moderate hepatic impairment, no significant changes were seen in the pharmacokinetics of nevirapine. However, a significant increase in the AUC of nevirapine observed in one patient with Child-Pugh Class B and ascites suggests that patients with worsening hepatic function and ascites may be at risk of accumulating nevirapine in the systemic circulation. Because nevirapine induces its own metabolism with multiple dosing, a single dose study may not reflect the impact of hepatic impairment on multiple dose pharmacokinetics (see PRECAUTIONS ). Nevirapine should not be administered to patients with severe hepatic impairment (see WARNINGS ).
Gender: In one Phase I study in healthy volunteers (15 females, 15 males), the weight-adjusted apparent volume of distribution (Vdss/F) of nevirapine was higher in the female subjects (1.54 L/kg) compared to the males (1.38 L/kg), suggesting that nevirapine was distributed more extensively in the female subjects. However, this difference was offset by a slightly shorter terminal-phase half-life in the females resulting in no significant gender difference in nevirapine oral clearance (24.6±7.7 mL/kg/hr in females vs. 19.9±3.9 mL/kg/hr in males after single dose) or plasma concentrations following either single- or multiple-dose administration(s).
Race: An evaluation of nevirapine plasma concentrations (pooled data from several clinical trials) from HIV-1 infected patients (27 Black, 24 Hispanic, 189 Caucasian) revealed no marked difference in nevirapine steady-state trough concentrations (median C minss = 4.7 µg/mL Black, 3.8 µg/mL Hispanic, 4.3 µg/mL Caucasian) with long-term nevirapine treatment at 400 mg/day. However, the pharmacokinetics of nevirapine have not been evaluated specifically for the effects of ethnicity.
Geriatric Patients: Nevirapine pharmacokinetics in HIV-1 infected adults do not appear to change with age (range 18-68 years); however, nevirapine has not been extensively evaluated in patients beyond the age of 55 years.
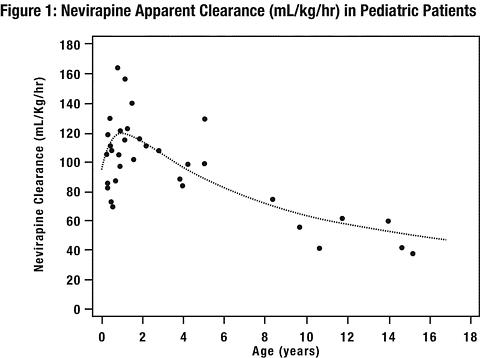
Pediatric Patients: The pharmacokinetics of nevirapine have been studied in two open-label studies in children with HIV-1 infection. In one study (BI 853; ACTG 165), nine HIV-1-infected children ranging in age from 9 months to 14 years were administered a single dose (7.5 mg, 30 mg, or 120 mg per m 2 ; n=3 per dose) of nevirapine suspension after an overnight fast. The mean nevirapine apparent clearance adjusted for body weight was greater in children compared to adults.
In a multiple dose study (BI 882; ACTG 180), nevirapine suspension or tablets (240 or 400 mg/m 2 /day) were administered as monotherapy or in combination with ZDV or ZDV+ddI to 37 HIV-1-infected pediatric patients with the following demographics: male (54%), racial minority groups (73%), median age of 11 months (range: 2 months-15 years). The majority of these patients received 120 mg/m 2 /day of nevirapine for approximately 4 weeks followed by 120 mg/m 2 /b.i.d. (patients > 9 years of age) or 200 mg/m 2 /b.i.d. (patients </= 9 years of age). Nevirapine apparent clearance adjusted for body weight reached maximum values by age 1 to 2 years and then decreased with increasing age. Nevirapine apparent clearance adjusted for body weight was at least two-fold greater in children younger than 8 years compared to adults. The relationship between nevirapine clearance with long term drug administration and age is shown in Figure 1. The pediatric dosing regimens were selected in order to achieve steady-state plasma concentrations in pediatric patients that approximate those in adults (see DOSAGE AND ADMINISTRATION , Pediatric Patients ).
Drug Interactions: (see PRECAUTIONS , Drug Interactions ) Nevirapine induces hepatic cytochrome P450 metabolic isoenzymes 3A4 and 2B6. Co-administration of VIRAMUNE and drugs primarily metabolized by CYP3A4 or CYP2B6 may result in decreased plasma concentrations of these drugs and attenuate their therapeutic effects.
While primarily an inducer of cytochrome P450 3A4 and 2B6 enzymes, nevirapine may also inhibit this system. Among human hepatic cytochrome P450s, nevirapine was capable in vitro of inhibiting the 10-hydroxylation of (R)-warfarin (CYP3A4). The estimated K i for the inhibition of CYP3A4 was 270 µM, a concentration that is unlikely to be achieved in patients as the therapeutic range is <25 µM. Therefore, nevirapine may have minimal inhibitory effect on other substrates of CYP3A4.
Nevirapine does not appear to affect the plasma concentrations of drugs that are substrates of other CYP450 enzyme systems, such as 1A2, 2D6, 2A6, 2E1, 2C9 or 2C19.
Table 1 (see below) contains the results of drug interaction studies performed with VIRAMUNE and other drugs likely to be co-administered. The effects of VIRAMUNE on the AUC, C max , and C min of co-administered drugs are summarized. To measure the full potential pharmacokinetic interaction effect following induction, patients on the concomitant drug at steady state were administered 28 days of VIRAMUNE (200 mg QD for 14 days followed by 200 mg BID for 14 days) followed by a steady state reassessment of the concomitant drug.
Table 1 Drug Interactions: Changes in Pharmacokinetic Parameters for Co-administered Drug
in the Presence of VIRAMUNE (All interaction studies were conducted in HIV-1 positive patients)Co-administered Drug Dose of
Co-administered DrugDose Regimen of VIRAMUNE n % Change of Co-administered Drug Pharmacokinetic Parameters (90% CI) Antiretrovirals AUC C max C min Didanosine 100-150 mg BID 200 mg QD × 14 days; 200 mg BID × 14 days 18 [iff ] [iff ] § Efavirenz a 600 mg QD 200 mg QD × 14 days; 400 mg QD × 14 days 17 down 28
( down 34 to down 14)down 12
( down 23 to up 1)down 32
( down 35 to down 19)Indinavir a 800 mg q8H 200 mg QD × 14 days; 200 mg BID × 14 days 19 down 31
( down 39 to down 22)down 15
( down 24 to down 4)down 44
( down 53 to down 33)Lopinavir a , b 300/75 mg/m 2 (lopinavir/ritonavir) b 7 mg/kg or 4 mg/kg QD × 2 weeks; BID × 1 week 12, 15 c down 14
( down 36 to up16)down 22
( down 44 to up 9)down 55
( down 75 to down 9)Lopinavir a 400/100 mg BID (lopinavir/ritonavir) 200 mg QD × 14 days; 200 mg BID > 1 year 22, 19 c down 27
( down 47 to down 2)down 19
( down 38 to up 5)down 51
( down 72 to down 26)Nelfinavir a 750 mg TID 200 mg QD × 14 days; 200 mg BID × 14 days 23 [iff ] [iff ] down 32
( down 50 to up 5)Nelfinavir-M8 metabolite down 62
( down 70 to down 53)down 59
( down 68 to down 48)down 66
( down 74 to down 55)Ritonavir 600 mg BID 200 mg QD × 14 days; 200 mg BID × 14 days 18 [iff ] [iff ] [iff ] Saquinavir a 600 mg TID 200 mg QD × 14 days; 200 mg BID × 21 days 23 down 38
( down 47 to down 11)down 32
( down 44 to down 6)§ Stavudine 30-40 mg BID 200 mg QD × 14 days; 200 mg BID × 14 days 22 [iff ] [iff ] § Zalcitabine 0.125-0.25 mg TID 200 mg QD × 14 days; 200 mg BID × 14 days 6 [iff ] [iff ] § Zidovudine 100-200 mg TID 200 mg QD × 14 days; 200 mg BID × 14 days 11 down 28
( down 40 to down 4)down 30
( down 51 to up 14)§ Other Medications AUC C max C min Clarithromycin a 500 mg BID 200 mg QD × 14 days; 200 mg BID × 14 days 15 down 31
( down 38 to down 24)down 23
( down 31 to down 14)down 57
( down 70 to down 36)Metabolite 14-OH-clarithromycin up 42
( up 16 to up 73)up 47
( up 21 to up 80)[iff ] Ethinyl estradiol a
and0.035 mg (as Ortho-Novum ® 1/35) 200 mg QD × 14 days; 200 mg BID × 14 days 10 down 20
( down 33 to down 3)[iff ] § Norethindrone a 1 mg (as Ortho-Novum ® 1/35) down 19
( down 30 to down 7)down 16
( down 27 to down 3)§ Fluconazole 200 mg QD 200 mg QD × 14 days; 200 mg BID × 14 days 19 [iff ] [iff ] [iff ] Ketoconazole a 400 mg QD 200 mg QD × 14 days; 200 mg BID × 14 days 21 down 72
( down 80 to down 60)down 44
( down 58 to down 27)§ Rifabutin a 150 or 300 mg QD 200 mg QD × 14 days; 200 mg BID × 14 days 19 up 17
( down 2 to up 40)up 28
( up 9 to up 51)[iff ] Metabolite 25-O-desacetyl-
rifabutinup 24
( down 16 to up 84)up 29
( down 2 to up 68)up 22
( down 14 to up 74)Rifampin a 600 mg QD 200 mg QD × 14 days; 200 mg BID × 14 days 14 up 11
( down 4 to up 28)[iff ] § § = C min below detectable level of the assay up = Increase, down = Decrease, [iff ] = No Effect a For information regarding clinical recommendations see PRECAUTIONS , Drug Interactions , Table 3 b Pediatric subjects ranging in age from 6 months to 12 years c Parallel group design; n for VIRAMUNE +lopinavir/ritonavir, n for lopinavir/ritonavir alone
Because of the design of the drug interaction trials (addition of 28 days of VIRAMUNE therapy to existing HIV therapy) the effect of the concomitant drug on plasma nevirapine steady state concentrations was estimated by comparison to historical controls.
Administration of rifampin had a clinically significant effect on nevirapine pharmacokinetics, decreasing AUC and C max by greater than 50%. Administration of fluconazole resulted in an approximate 100% increase in nevirapine exposure, based on a comparison to historic data (see PRECAUTIONS , Drug Interactions , Table 3 ). The effect of other drugs listed in Table 1 on nevirapine pharmacokinetics was not significant.
INDICATIONS AND USAGE
VIRAMUNE (nevirapine) is indicated for use in combination with other antiretroviral agents for the treatment of HIV-1 infection. This indication is based on one principal clinical trial (BI 1090) that demonstrated prolonged suppression of HIV-RNA and two smaller supportive studies, one of which (BI 1046) is described below.
Additional important information regarding the use of VIRAMUNE for the treatment of HIV-1 infection:
- Based on serious and life-threatening hepatotoxicity observed in controlled and uncontrolled studies, VIRAMUNE should not be initiated in adult females with CD4+ cell counts greater than 250 cells/mm 3 or in adult males with CD4+ cell counts greater than 400 cells/mm 3 unless the benefit outweighs the risk (see WARNINGS ).
- The 14-day lead-in period with VIRAMUNE 200 mg daily dosing has been demonstrated to reduce the frequency of rash (see WARNINGS ; DOSAGE AND ADMINISTRATION ).
Description of Clinical Studies:Trial BI 1090, was a placebo-controlled, double-blind, randomized trial in 2249 HIV-1 infected patients with <200 CD4+ cells at screening. Initiated in 1995, BI 1090 compared treatment with VIRAMUNE + lamivudine + background therapy versus lamivudine + background therapy in NNRTI na[iuml ]ve patients. Treatment doses were VIRAMUNE, 200 mg daily for two weeks followed by 200 mg twice daily or placebo, and lamivudine 150 mg twice daily. Other antiretroviral agents were given at approved doses. Initial background therapy (in addition to lamivudine) was one NRTI in 1309 patients (58%), two or more NRTIs in 771 (34%), and PIs and NRTIs in 169 (8%). The patients (median age 36.5 years, 70% Caucasian, 79% male) had advanced HIV infection, with a median baseline CD4+ cell count of 96 cells/mm 3 and a baseline HIV RNA of 4.58 log 10 copies/mL (38,291 copies/mL). Prior to entering the trial, 45% had previously experienced an AIDS-defining clinical event. Eighty-nine percent had antiretroviral treatment prior to entering the trial. BI 1090 was originally designed as a clinical endpoint study. Prior to unblinding the trial, the primary endpoint was changed to proportion of patients with HIV RNA <50 copies/mL and not previously failed at 48 weeks. Treatment response and outcomes are shown in Table 2.
Table 2 BI 1090 Outcomes through 48 weeks OutcomeVIRAMUNE
(N=1121)
%Placebo
(N=1128)
%Responders at 48 weeks:
HIV RNA <50 copies/mL18.0 1.6 Treatment Failure82.0 98.4 Never suppressed viral load44.6 66.4 Virologic failure after response7.2 4.3 CDC category C event or
death9.6 11.2 Added antiretroviral therapy 1
while <50 copies/mL5.0 0.9 Discontinued trial therapy due
to AE7.0 5.9 Discontinued trial <48 weeks 28.5 9.8 1 including change to open-label NVP2 includes withdrawal of consent, lost to follow-up, non-compliance with protocol, other administrative reasons
The change from baseline in CD4+ cell count through one year of therapy was significantly greater for the VIRAMUNE group compared to the placebo group for the overall study population (64 cells/mm 3 vs 22 cells/mm 3 , respectively), as well as for patients who entered the trial as treatment na[iuml ]ve or having received only ZDV (85 cells/mm 3 vs 25 cells/mm 3 , respectively).
At two years into the study, 16% of subjects on VIRAMUNE had experienced class C CDC events as compared to 21% of subjects on the control arm.
Trial BI 1046 (INCAS) was a double-blind, placebo-controlled, randomized, three arm trial with 151 HIV-1 infected patients with CD4+ cell counts of 200-600 at baseline. BI 1046 compared treatment with VIRAMUNE+zidovudine+didanosine to VIRAMUNE+zidovudine and zidovudine+didanosine. Treatment doses were VIRAMUNE at 200 mg daily for two weeks followed by 200 mg twice daily or placebo, zidovudine at 200 mg three times daily, and didanosine at 125 or 200 mg twice daily (depending on body weight). The patients had mean baseline HIV RNA of 4.41 log 10 copies/mL (25,704 copies/mL) and mean baseline CD4+ cell count of 376 cells/mm 3 . The primary endpoint was the proportion of patients with HIV-RNA < 400 copies/mL and not previously failed at 48 weeks. The virologic responder rates at 48 weeks were 45% for patients treated with VIRAMUNE+zidovudine+didanosine, 19% for patients treated with zidovudine+didanosine, and 0% for patients treated with VIRAMUNE+zidovudine.
CD4+ cell counts in the VIRAMUNE+ZDV+ddI group increased above baseline by a mean of 139 cells/mm 3 at one year, significantly greater than the increase of 87 cells/mm 3 in the ZDV+ddI patients. The VIRAMUNE+ZDV group mean decreased by 6 cells/mm 3 below baseline.
CONTRAINDICATIONS
VIRAMUNE (nevirapine) is contraindicated in patients with clinically significant hypersensitivity to any of the components contained in the tablet or the oral suspension.
WARNINGS
General:
The most serious adverse reactions associated with VIRAMUNE (nevirapine) are hepatitis/hepatic failure, Stevens-Johnson syndrome, toxic epidermal necrolysis, and hypersensitivity reactions. Hepatitis/hepatic failure may be associated with signs of hypersensitivity which can include severe rash or rash accompanied by fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, facial edema, eosinophilia, granulocytopenia, lymphadenopathy, or renal dysfunction.
The first 18 weeks of therapy with VIRAMUNE are a critical period during which intensive clinical and laboratory monitoring of patients is required to detect potentially life-threatening hepatic events and skin reactions. The optimal frequency of monitoring during this time period has not been established. Some experts recommend clinical and laboratory monitoring more often than once per month, and in particular, would include monitoring of liver function tests at baseline, prior to dose escalation and at two weeks post-dose escalation. After the initial 18 week period, frequent clinical and laboratory monitoring should continue throughout VIRAMUNE treatment. In addition, the 14-day lead-in period with VIRAMUNE 200 mg daily dosing has been demonstrated to reduce the frequency of rash.
Hepatic Events:
Severe, life-threatening, and in some cases fatal hepatotoxicity, including fulminant and cholestatic hepatitis, hepatic necrosis and hepatic failure, have been reported in patients treated with VIRAMUNE. In controlled clinical trials, symptomatic hepatic events regardless of severity occurred in 4% (range 0% to 11.0%) of patients who received VIRAMUNE and 1.2% of patients in control groups.
The risk of symptomatic hepatic events regardless of severity was greatest in the first 6 weeks of therapy. The risk continued to be greater in the VIRAMUNE groups compared to controls through 18 weeks of treatment. However, hepatic events may occur at any time during treatment. In some cases, patients presented with non-specific, prodromal signs or symptoms of fatigue, malaise, anorexia, nausea, jaundice, liver tenderness or hepatomegaly, with or without initially abnormal serum transaminase levels. Rash was observed in approximately half of the patients with symptomatic hepatic adverse events. Fever and flu-like symptoms accompanied some of these hepatic events. Some events, particularly those with rash and other symptoms, have progressed to hepatic failure with transaminase elevation, with or without hyperbilirubinemia, hepatic encephalopathy, prolonged partial thromboplastin time, or eosinophilia. Patients with signs or symptoms of hepatitis must be advised to discontinue VIRAMUNE and immediately seek medical evaluation, which should include liver function tests.
Liver function tests should be performed immediately if a patient experiences signs or symptoms suggestive of hepatitis and/or hypersensitivity reaction. Liver function tests should also be obtained immediately for all patients who develop a rash in the first 18 weeks of treatment. Physicians and patients should be vigilant for the appearance of signs or symptoms of hepatitis, such as fatigue, malaise, anorexia, nausea, jaundice, bilirubinuria, acholic stools, liver tenderness or hepatomegaly. The diagnosis of hepatotoxicity should be considered in this setting, even if liver function tests are initially normal or alternative diagnoses are possible (see PRECAUTIONS , Information for Patients ; DOSAGE AND ADMINISTRATION ).
If clinical hepatitis or transaminase elevations combined with rash or other systemic symptoms occur, VIRAMUNE should be permanently discontinued. Do not restart VIRAMUNE after recovery. In some cases, hepatic injury progresses despite discontinuation of treatment.
The patients at greatest risk of hepatic events, including potentially fatal events, are women with high CD4 counts. In general, during the first 6 weeks of treatment, women have a three fold higher risk than men for symptomatic, often rash-associated, hepatic events (5.8% versus 2.2%), and patients with higher CD4 counts at initiation of VIRAMUNE therapy are at higher risk for symptomatic hepatic events with VIRAMUNE. In a retrospective review, women with CD4 counts >250 cells/mm 3 had a 12 fold higher risk of symptomatic hepatic adverse events compared to women with CD4 counts <250 cells/mm 3 (11.0% versus 0.9%). An increased risk was observed in men with CD4 counts >400 cells/mm 3 (6.3% versus 1.2% for men with CD4 counts <400 cells/mm 3 ). However, all patients, regardless of gender, CD4 count, or antiretroviral treatment history, should be monitored for hepatotoxicity since symptomatic hepatic adverse events have been reported at all CD4 counts. Co-infection with hepatitis B or C and/or increased liver function tests at the start of therapy with VIRAMUNE® are associated with a greater risk of later symptomatic events (6 weeks or more after starting VIRAMUNE) and asymptomatic increases in AST or ALT.
In addition, serious hepatotoxicity (including liver failure requiring transplantation in one instance) has been reported in HIV-uninfected individuals receiving multiple doses of VIRAMUNE in the setting of post-exposure prophylaxis, an unapproved use.
Because increased nevirapine levels and nevirapine accumulation may be observed in patients with serious liver disease, VIRAMUNE should not be administered to patients with severe hepatic impairment (see CLINICAL PHARMACOLOGY , Pharmacokinetics in Special Populations : Hepatic Impairment; PRECAUTIONS , General ).
Skin Reactions:
Severe and life-threatening skin reactions, including fatal cases, have been reported, occurring most frequently during the first 6 weeks of therapy. These have included cases of Stevens-Johnson syndrome, toxic epidermal necrolysis, and hypersensitivity reactions characterized by rash, constitutional findings, and organ dysfunction including hepatic failure. In controlled clinical trials, Grade 3 and 4 rashes were reported during the first 6 weeks in 1.5% of VIRAMUNE recipients compared to 0.1% of placebo subjects.
Patients developing signs or symptoms of severe skin reactions or hypersensitivity reactions (including, but not limited to, severe rash or rash accompanied by fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, facial edema, and/or hepatitis, eosinophilia, granulocytopenia, lymphadenopathy, and renal dysfunction) must permanently discontinue VIRAMUNE and seek medical evaluation immediately (see PRECAUTIONS , Information for Patients ). Do not restart VIRAMUNE following severe skin rash, skin rash combined with increased transaminases or other symptoms, or hypersensitivity reaction.
If patients present with a suspected VIRAMUNE-associated rash, liver function tests should be performed. Patients with rash-associated AST or ALT elevations should be permanently discontinued from VIRAMUNE.
Therapy with VIRAMUNE must be initiated with a 14-day lead-in period of 200 mg/day (4 mg/kg/day in pediatric patients), which has been shown to reduce the frequency of rash. If rash is observed during this lead-in period, dose escalation should not occur until the rash has resolved (see DOSAGE AND ADMINISTRATION ). Patients should be monitored closely if isolated rash of any severity occurs. Delay in stopping VIRAMUNE treatment after the onset of rash may result in a more serious reaction.
Women appear to be at higher risk than men of developing rash with VIRAMUNE.
In a clinical trial, concomitant prednisone use (40 mg/day for the first 14 days of VIRAMUNE administration) was associated with an increase in incidence and severity of rash during the first 6 weeks of VIRAMUNE therapy. Therefore, use of prednisone to prevent VIRAMUNE-associated rash is not recommended.
Resistance
VIRAMUNE must not be used as a single agent to treat HIV or added on as a sole agent to a failing regimen. As with all other non-nucleoside reverse transcriptase inhibitors, resistant virus emerges rapidly when nevirapine is administered as monotherapy. The choice of new antiretroviral agents to be used in combination with nevirapine should take into consideration the potential for cross resistance. When discontinuing an antiretroviral regimen containing VIRAMUNE, the long half-life of nevirapine should be taken into account; if antiretrovirals with shorter half-lives than VIRAMUNE are stopped concurrently, low plasma concentrations of nevirapine alone may persist for a week or longer and virus resistance may subsequently develop.
St. John's wort:
Concomitant use of St. John's wort (hypericum perforatum) or St. John's wort containing products and VIRAMUNE is not recommended. Co-administration of non-nucleoside reverse transcriptase inhibitors (NNRTIs), including VIRAMUNE, with St. John's wort is expected to substantially decrease NNRTI concentrations and may result in sub-optimal levels of VIRAMUNE and lead to loss of virologic response and possible resistance to VIRAMUNE or to the class of NNRTIs.
PRECAUTIONS
General:
The most serious adverse reactions associated with VIRAMUNE (nevirapine) are hepatitis/hepatic failure, Stevens-Johnson syndrome, toxic epidermal necrolysis, and hypersensitivity reactions. Hepatitis/hepatic failure may be isolated or associated with signs of hypersensitivity which may include severe rash or rash accompanied by fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, facial edema, eosinophilia, granulocytopenia, lymphadenopathy, or renal dysfunction (see WARNINGS ).
Nevirapine is extensively metabolized by the liver and nevirapine metabolites are extensively eliminated by the kidney. No adjustment in nevirapine dosing is required in patients with CrCL >/=20 mL/min. In patients undergoing chronic hemodialysis, an additional 200 mg dose following each dialysis treatment is indicated. Nevirapine metabolites may accumulate in patients receiving dialysis; however, the clinical significance of this accumulation is not known (see CLINICAL PHARMACOLOGY , Pharmacokinetics in Special Populations : Renal Impairment; DOSAGE AND ADMINISTRATION , Dosage Adjustment ).
It is not clear whether a dosing adjustment is needed for patients with mild to moderate hepatic impairment, because multiple dose pharmacokinetic data are not available for this population. However, patients with moderate hepatic impairment and ascites may be at risk of accumulating nevirapine in the systemic circulation. Caution should be exercised when nevirapine is administered to patients with moderate hepatic impairment. Nevirapine should not be administered to patients with severe hepatic impairment (see WARNINGS ; CLINICAL PHARMACOLOGY , Pharmacokinetics in Special Populations : Hepatic Impairment) .
The duration of clinical benefit from antiretroviral therapy may be limited. Patients receiving VIRAMUNE or any other antiretroviral therapy may continue to develop opportunistic infections and other complications of HIV infection, and therefore should remain under close clinical observation by physicians experienced in the treatment of patients with associated HIV diseases.
When administering VIRAMUNE as part of an antiretroviral regimen, the complete product information for each therapeutic component should be consulted before initiation of treatment.
Drug Interactions:
Nevirapine is principally metabolized by the liver via the cytochrome P450 isoenzymes, 3A4 and 2B6. Nevirapine is known to be an inducer of these enzymes. As a result, drugs that are metabolized by these enzyme systems may have lower than expected plasma levels when co-administered with nevirapine.
The specific pharmacokinetic changes that occur with co-administration of nevirapine and other drugs are listed in CLINICAL PHARMACOLOGY , Table 1. Clinical comments about possible dosage modifications based on these pharmacokinetic changes are listed in Table 3. The data in Tables 1 and 3 are based on the results of drug interaction studies conducted in HIV-1 seropositive subjects unless otherwise indicated.
In addition to established drug interactions, there may be potential pharmacokinetic interactions between nevirapine and other drug classes that are metabolized by the cytochrome P450 system. These potential drug interactions are listed in Table 4. Although specific drug interaction studies in HIV-1 seropositive subjects have not been conducted for the classes of drugs listed in Table 4, additional clinical monitoring may be warranted when co-administering these drugs.
The in vitro interaction between nevirapine and the antithrombotic agent warfarin is complex. As a result, when giving these drugs concomitantly, plasma warfarin levels may change with the potential for increases in coagulation time. When warfarin is co-administered with nevirapine, anticoagulation levels should be monitored frequently.
Table 3 Established Drug Interactions: Alteration in Dose or Regimen May Be Recommended Based on Drug Interaction Studies (See CLINICAL PHARMACOLOGY , Table 1 for Magnitude of Interaction) Drug NameEffect on Concentration of Nevirapine or Concomitant DrugClinical CommentClarithromycindown Clarithromycin
up14-OH clarithromycinClarithromycin exposure was significantly decreased by nevirapine; however, 14-OH metabolite concentrations were increased. Because clarithromycin active metabolite has reduced activity against Mycobacterium avium-intracellulare complex , overall activity against this pathogen may be altered. Alternatives to clarithromycin, such as azithromycin, should be considered.Efavirenzdown EfavirenzAppropriate doses for this combination are not established.Ethinyl estradiol and Norethindronedown Ethinyl estradiol
down NorethindroneOral contraceptives and other hormonal methods of birth control should not be used as the sole method of contraception in women taking nevirapine, since nevirapine may lower the plasma levels of these medications. An alternative or additional method of contraception is recommended.Fluconazoleup NevirapineBecause of the risk of increased exposure to nevirapine, caution should be used in concomitant administration, and patients should be monitored closely for nevirapine-associated adverse events.Indinavirdown IndinavirAppropriate doses for this combination are not established, but an increase in the dosage of indinavir may be required.Ketoconazoledown KetoconazoleNevirapine and ketoconazole should not be administered concomitantly because decreases in ketoconazole plasma concentrations may reduce the efficacy of the drug.Lopinavir/Ritonavirdown LopinavirA dose increase of lopinavir/ritonavir to 533/133 mg twice daily with food is recommended in combination with nevirapine.Methadonedown Methadone aMethadone levels may be decreased; increased dosages may be required to prevent symptoms of opiate withdrawal. Methadone maintained patients beginning nevirapine therapy should be monitored for evidence of withdrawal and methadone dose should be adjusted accordingly.Nelfinavirdown Nelfinavir M8 Metabolite
down Nelfinavir C minThe appropriate dose for nelfinavir in combination with nevirapine, with respect to safety and efficacy, has not been established.Rifabutinup RifabutinRifabutin and its metabolite concentrations were moderately increased. Due to high intersubject variability, however, some patients may experience large increases in rifabutin exposure and may be at higher risk for rifabutin toxicity. Therefore, caution should be used in concomitant administration.Rifampindown NevirapineNevirapine and rifampin should not be administered concomitantly because decreases in nevirapine plasma concentrations may reduce the efficacy of the drug. Physicians needing to treat patients co-infected with tuberculosis and using a nevirapine containing regimen may use rifabutin instead.Saquinavirdown SaquinavirAppropriate doses for this combination are not established, but an increase in the dosage of saquinavir may be required.a Based on reports of narcotic withdrawal syndrome in patients treated with nevirapine and methadone concurrently, and evidence of decreased plasma concentrations of methadone.Table 4 Potential Drug Interactions: Use With Caution, Dose Adjustment of Co-administered Drug May Be
Needed due to Possible Decrease in Clinical EffectExamples of Drugs in Which Plasma Concentrations May Be Decreased By Co-administration With NevirapineDrug ClassExamples of DrugsAntiarrhythmicsAmiodarone, disopyramide, lidocaineAnticonvulsantsCarbamazepine, clonazepam, ethosuximideAntifungalsItraconazoleCalcium channel blockersDiltiazem, nifedipine, verapamilCancer chemotherapyCyclophosphamideErgot alkaloidsErgotamineImmunosuppressantsCyclosporin, tacrolimus, sirolimusMotility agentsCisaprideOpiate agonistsFentanylExamples of Drugs in Which Plasma Concentrations May Be Increased By Co-administration With NevirapineAntithromboticsWarfarin
Potential effect on anticoagulation. Monitoring of anticoagulation levels is recommended.Fat redistribution: Redistribution/accumulation of body fat including central obesity, dorsocervical fat enlargement (buffalo hump), peripheral wasting, facial wasting, breast enlargement, and "cushingoid appearance" have been observed in patients receiving antiretroviral therapy. The mechanism and long-term consequences of these events are currently unknown. A causal relationship has not been established.
Information for Patients:
Patients should be informed of the possibility of severe liver disease or skin reactions associated with VIRAMUNE that may result in death. Patients developing signs or symptoms of liver disease or severe skin reactions should be instructed to discontinue VIRAMUNE and seek medical attention immediately, including performance of laboratory monitoring. Symptoms of liver disease include fatigue, malaise, anorexia, nausea, jaundice, acholic stools, liver tenderness or hepatomegaly. Symptoms of severe skin or hypersensitivity reactions include rash accompanied by fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, facial edema and/or hepatitis.
Intensive clinical and laboratory monitoring, including liver function tests, is essential during the first 18 weeks of therapy with VIRAMUNE to detect potentially life-threatening hepatotoxicity and skin reactions. However, liver disease can occur after this period, therefore monitoring should continue at frequent intervals throughout VIRAMUNE treatment. Extra vigilance is warranted during the first 6 weeks of therapy, which is the period of greatest risk of hepatic events and skin reactions. Patients with signs and symptoms of hepatitis should discontinue VIRAMUNE and seek medical evaluation immediately. If VIRAMUNE is discontinued due to hepatotoxicity, do not restart it. Patients, particularly women, with increased CD4+ cell count at initiation of VIRAMUNE therapy (>250 cells/mm 3 in women and >400 cells/mm 3 in men) are at substantially higher risk for development of symptomatic hepatic events, often associated with rash. Patients should be advised that co-infection with hepatitis B or C and/or increased liver function tests at the start of therapy with VIRAMUNE are associated with a greater risk of later symptomatic events (6 weeks or more after starting VIRAMUNE) and asymptomatic increases in AST or ALT (see WARNINGS , Hepatic Events ).
The majority of rashes associated with VIRAMUNE occur within the first 6 weeks of initiation of therapy. Patients should be instructed that if any rash occurs during the two-week lead-in period, the VIRAMUNE dose should not be escalated until the rash resolves. Any patient experiencing a rash should have their liver function evaluated immediately. Patients with severe rash or hypersensitivity reactions should discontinue VIRAMUNE immediately and consult a physician. VIRAMUNE should not be restarted following severe skin rash or hypersensitivity reaction. Women tend to be at higher risk for development of VIRAMUNE associated rash.
Oral contraceptives and other hormonal methods of birth control should not be used as the sole method of contraception in women taking VIRAMUNE, since nevirapine may lower the plasma levels of these medications. Additionally, when oral contraceptives are used for hormonal regulation during VIRAMUNE therapy, the therapeutic effect of the hormonal therapy should be monitored (see PRECAUTIONS , Drug Interactions ).
Based on the known metabolism of methadone, nevirapine may decrease plasma concentrations of methadone by increasing its hepatic metabolism. Narcotic withdrawal syndrome has been reported in patients treated with VIRAMUNE and methadone concomitantly. Methadone- maintained patients beginning nevirapine therapy should be monitored for evidence of withdrawal and methadone dose should be adjusted accordingly.
VIRAMUNE may interact with some drugs, therefore, patients should be advised to report to their doctor the use of any other prescription, non-prescription medication or herbal products, particularly St. John's wort.
Patients should be informed that VIRAMUNE therapy has not been shown to reduce the risk of transmission of HIV-1 to others through sexual contact or blood contamination. The long-term effects of VIRAMUNE are unknown at this time.
VIRAMUNE is not a cure for HIV-1 infection; patients may continue to experience illnesses associated with advanced HIV-1 infection, including opportunistic infections. Patients should be advised to remain under the care of a physician when using VIRAMUNE.
Patients should be informed to take VIRAMUNE every day as prescribed. Patients should not alter the dose without consulting their doctor. If a dose is missed, patients should take the next dose as soon as possible. However, if a dose is skipped, the patient should not double the next dose. Patients should be advised to report to their doctor the use of any other medications.
Patients should be informed that redistribution or accumulation of body fat may occur in patients receiving antiretroviral therapy and that the cause and long term health effects of these conditions are not known at this time.
The Medication Guide provides written information for the patient, and should be dispensed with each new prescription and refill.
Carcinogenesis, Mutagenesis, Impairment of Fertility:
Long-term carcinogenicity studies in mice and rats were carried out with nevirapine. Mice were dosed with 0, 50, 375 or 750 mg/kg/day for two years. Hepatocellular adenomas and carcinomas were increased at all doses in males and at the two high doses in females. In studies in which rats were administered nevirapine at doses of 0, 3.5, 17.5 or 35 mg/kg/day for two years, an increase in hepatocellular adenomas was seen in males at all doses and in females at the high dose. The systemic exposure (based on AUCs) at all doses in the two animal studies were lower than that measured in humans at the 200 mg bid dose. The mechanism of the carcinogenic potential is unknown. However, in genetic toxicology assays, nevirapine showed no evidence of mutagenic or clastogenic activity in a battery of in vitro and in vivo studies. These included microbial assays for gene mutation (Ames: Salmonella strains and E. coli ), mammalian cell gene mutation assay (CHO/HGPRT), cytogenetic assays using a Chinese hamster ovary cell line and a mouse bone marrow micronucleus assay following oral administration. Given the lack of genotoxic activity of nevirapine, the relevance to humans of hepatocellular neoplasms in nevirapine treated mice and rats is not known. In reproductive toxicology studies, evidence of impaired fertility was seen in female rats at doses providing systemic exposure, based on AUC, approximately equivalent to that provided with the recommended clinical dose of VIRAMUNE.
Pregnancy: Pregnancy Category C
No observable teratogenicity was detected in reproductive studies performed in pregnant rats and rabbits. In rats, a significant decrease in fetal body weight occurred at doses providing systemic exposure approximately 50% higher, based on AUC, than that seen at the recommended human clinical dose.
The maternal and developmental no-observable-effect level dosages in rats and rabbits produced systemic exposures approximately equivalent to or approximately 50% higher, respectively, than those seen at the recommended daily human dose, based on AUC. There are no adequate and well-controlled studies in pregnant women. VIRAMUNE should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Severe hepatic events, including fatalities, have been reported in pregnant women receiving chronic VIRAMUNE therapy as part of combination treatment of HIV infection. It is unclear if pregnancy augments the already increased risk observed in non-pregnant women (see Boxed WARNING ).
Antiretroviral Pregnancy Registry:
To monitor maternal-fetal outcomes of pregnant women exposed to VIRAMUNE, an Antiretroviral Pregnancy Registry has been established. Physicians are encouraged to register patients by calling (800) 258-4263.
Nursing Mothers:
The Centers for Disease Control and Prevention recommend that HIV-infected mothers not breast-feed their infants to avoid risking postnatal transmission of HIV. Nevirapine is excreted in breast milk. Because of both the potential for HIV transmission and the potential for serious adverse reactions in nursing infants, mothers should be instructed not to breast-feed if they are receiving VIRAMUNE.
Pediatric Use:
The pharmacokinetics of nevirapine have been studied in two open-label studies in children with HIV-1 infection (see CLINICAL PHARMACOLOGY , Pharmacokinetics in Special Populations ). For dose recommendations for pediatric patients see DOSAGE AND ADMINISTRATION . The most frequently reported adverse events related to VIRAMUNE in pediatric patients were similar to those observed in adults, with the exception of granulocytopenia, which was more commonly observed in children receiving both zidovudine and VIRAMUNE (see ADVERSE REACTIONS , Pediatric Patients ). The evaluation of the antiviral activity of VIRAMUNE in pediatric patients is ongoing.
Geriatric Use:
Clinical studies of VIRAMUNE did not include sufficient numbers of subjects aged 65 and older to determine whether elderly subjects respond differently from younger subjects. In general, dose selection for an elderly patient should be cautious, reflecting the greater frequency of decreased hepatic, renal or cardiac function, and of concomitant disease or other drug therapy.
ADVERSE REACTIONS
The most serious adverse reactions associated with VIRAMUNE (nevirapine) are hepatitis/hepatic failure, Stevens-Johnson syndrome, toxic epidermal necrolysis, and hypersensitivity reactions. Hepatitis/hepatic failure may be isolated or associated with signs of hypersensitivity which may include severe rash or rash accompanied by fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, facial edema, eosinophilia, granulocytopenia, lymphadenopathy, or renal dysfunction (see WARNINGS ).
Adults:
The most common clinical toxicity of VIRAMUNE is rash, which can be severe or life-threatening (see WARNINGS ). Rash occurs most frequently within the first 6 weeks of therapy. Rashes are usually mild to moderate, maculopapular erythematous cutaneous eruptions, with or without pruritus, located on the trunk, face and extremities. In controlled clinical trials, Grade 1 and 2 rashes were reported in 13.3% of patients receiving VIRAMUNE compared to 5.8% receiving placebo during the first 6 weeks of therapy. Grade 3 and 4 rashes were reported in 1.5% of VIRAMUNE recipients compared to 0.1% of subjects receiving placebo. Women tend to be at higher risk for development of VIRAMUNE associated rash.
In controlled clinical trials, symptomatic hepatic events regardless of severity occurred in 4.0% (range 0% to 11.0%) of patients who received VIRAMUNE and 1.2% of patients in control groups. Female gender and higher CD4 counts (>250 cells/mm 3 in women and >400 cells/mm 3 in men) place patients at increased risk of these events (see WARNINGS ).
Asymptomatic transaminase elevations (AST or ALT > 5X ULN) were observed in 5.8% (range 0% to 9.2%) of patients who received VIRAMUNE and 5.5% of patients in control groups. Co-infection with hepatitis B or C and/or increased liver function tests at the start of therapy with VIRAMUNE are associated with a greater risk of later symptomatic events (6 weeks or more after starting VIRAMUNE) and asymptomatic increases in AST or ALT.
Treatment related, adverse experiences of moderate or severe intensity observed in >2% of patients receiving VIRAMUNE in placebo-controlled trials are shown in Table 5.
Table 5 Percentage of Patients with Moderate or Severe Drug Related Events
in Adult Placebo Controlled TrialsTrial 1090 1 Trials 1037, 1038, 1046 2 VIRAMUNE Placebo VIRAMUNE Placebo (n=1121) (n=1128) (n=253) (n=203) Median exposure (weeks)58 52 28 28 Any adverse event14.5% 11.1% 31.6% 13.3% Rash5.1 1.8 6.7 1.5 Nausea0.5 1.1 8.7 3.9 Granulocytopenia1.8 2.8 0.4 0 Headache0.7 0.4 3.6 0.5 Fatigue0.2 0.3 4.7 3.9 Diarrhea0.2 0.8 2.0 0.5 Abdominal pain0.1 0.4 2.0 0 Myalgia0.2 0 1.2 2.0 1 Background therapy included 3TC for all patients and combinations of NRTIs and PIs. Patients had CD4+ cell counts <200 cells/mm 3 .2 Background therapy included ZDV and ZDV+ddI; VIRAMUNE monotherapy was administered in some patients. Patients had CD4+ cell count >/=200 cells/mm 3 .Laboratory Abnormalities: Liver function test abnormalities (AST, ALT) were observed more frequently in patients receiving VIRAMUNE than in controls (Table 6). Asymptomatic elevations in GGT occur frequently but are not a contraindication to continue VIRAMUNE therapy in the absence of elevations in other liver function tests. Other laboratory abnormalities (bilirubin, anemia, neutropenia, thrombocytopenia) were observed with similar frequencies in clinical trials comparing VIRAMUNE and control regimens (see Table 6).
Table 6 Percentage of Adult Patients with Laboratory Abnormalities Trial 1090 1 Trials 1037, 1038, 1046 2 VIRAMUNE Placebo VIRAMUNE Placebo Laboratory Abnormalityn=1121 n=1128 n=253 n=203 Blood ChemistrySGPT (ALT) >250 U/L5.3% 4.4% 14.0% 4.0% SGOT (AST) >250 U/L3.7 2.5 7.6 1.5 Bilirubin >2.5 mg/dL1.7 2.2 1.7 1.5 HematologyHemoglobin <8.0 g/dL3.2 4.1 0 0 Platelets <50,000/mm 31.3 1.0 0.4 1.5 Neutrophils <750/mm 313.3 13.5 3.6 1.0 1 Background therapy included 3TC for all patients and combinations of NRTIs and PIs. Patients had CD4+ cell counts <200 cells/mm 3 .2 Background therapy included ZDV and ZDV+ddI; VIRAMUNE monotherapy was administered in some patients. Patients had CD4+ cell count >/=200 cells/mm 3 .Post Marketing Surveillance: In addition to the adverse events identified during clinical trials, the following events have been reported with the use of VIRAMUNE in clinical practice:
Body as a Whole: fever, somnolence, drug withdrawal (see PRECAUTIONS : Drug Interactions ), redistribution/accumulation of body fat (see PRECAUTIONS , Fat redistribution )
Gastrointestinal: vomiting
Liver and Biliary: jaundice, fulminant and cholestatic hepatitis, hepatic necrosis, hepatic failure
Hematology: anemia, eosinophilia, neutropenia
Musculoskeletal: arthralgia
Neurologic: paraesthesia
Skin and Appendages: allergic reactions including anaphylaxis, angioedema, bullous eruptions, ulcerative stomatitis and urticaria have all been reported. In addition, hypersensitivity syndrome and hypersensitivity reactions with rash associated with constitutional findings such as fever, blistering, oral lesions, conjunctivitis, facial edema, muscle or joint aches, general malaise, fatigue or significant hepatic abnormalities (see WARNINGS ) plus one or more of the following: hepatitis, eosinophilia, granulocytopenia, lymphadenopathy and/or renal dysfunction have been reported with the use of VIRAMUNE.
Pediatric Patients:
Safety was assessed in trial BI 882 in which patients were followed for a mean duration of 33.9 months (range: 6.8 months to 5.3 years, including long-term follow-up in 29 of these patients in trial BI 892). The most frequently reported adverse events related to VIRAMUNE in pediatric patients were similar to those observed in adults, with the exception of granulocytopenia, which was more commonly observed in children receiving both zidovudine and VIRAMUNE. Serious adverse events were assessed in ACTG 245, a double-blind, placebo-controlled trial of VIRAMUNE (n = 305) in which pediatric patients received combination treatment with VIRAMUNE. In this trial two patients were reported to experience Stevens-Johnson syndrome or Stevens-Johnson/toxic epidermal necrolysis transition syndrome. Cases of allergic reaction, including one case of anaphylaxis, were also reported.
OVERDOSAGE
There is no known antidote for VIRAMUNE (nevirapine) overdosage. Cases of VIRAMUNE overdose at doses ranging from 800 to 1800 mg per day for up to 15 days have been reported. Patients have experienced events including edema, erythema nodosum, fatigue, fever, headache, insomnia, nausea, pulmonary infiltrates, rash, vertigo, vomiting and weight decrease. All events subsided following discontinuation of VIRAMUNE.
DOSAGE AND ADMINISTRATION
Adults:
The recommended dose for VIRAMUNE (nevirapine) is one 200 mg tablet daily for the first 14 days (this lead-in period should be used because it has been found to lessen the frequency of rash) , followed by one 200 mg tablet twice daily, in combination with other antiretroviral agents. For concomitantly administered antiretroviral therapy, the manufacturer's recommended dosage and monitoring should be followed.
Pediatric Patients:
The recommended oral dose of VIRAMUNE for pediatric patients 2 months up to 8 years of age is 4 mg/kg once daily for the first 14 days followed by 7 mg/kg twice daily thereafter. For patients 8 years and older the recommended dose is 4 mg/kg once daily for two weeks followed by 4 mg/kg twice daily thereafter. The total daily dose should not exceed 400 mg for any patient.
VIRAMUNE suspension should be shaken gently prior to administration. It is important to administer the entire measured dose of suspension by using an oral dosing syringe or dosing cup. An oral dosing syringe is recommended, particularly for volumes of 5 mL or less. If a dosing cup is used, it should be thoroughly rinsed with water and the rinse should also be administered to the patient.
Monitoring of Patients:
Intensive clinical and laboratory monitoring, including liver function tests, is essential at baseline and during the first 18 weeks of treatment with VIRAMUNE. The optimal frequency of monitoring during this period has not been established. Some experts recommend clinical and laboratory monitoring more often than once per month, and in particular, would include monitoring of liver function tests at baseline, prior to dose escalation, and at two weeks post dose escalation. After the initial 18 week period, frequent clinical and laboratory monitoring should continue throughout VIRAMUNE treatment (see WARNINGS ). In some cases, hepatic injury has progressed despite discontinuation of treatment.
Dosage Adjustment:
VIRAMUNE should be discontinued if patients experience severe rash or a rash accompanied by constitutional findings (see WARNINGS ). Patients experiencing rash during the 14-day lead-in period of 200 mg/day (4 mg/kg/day in pediatric patients) should not have their VIRAMUNE dose increased until the rash has resolved (see PRECAUTIONS , Information for Patients ).
If a clinical (symptomatic) hepatic event occurs, VIRAMUNE should be permanently discontinued. Do not restart VIRAMUNE after recovery (see WARNINGS ).
Patients who interrupt VIRAMUNE dosing for more than 7 days should restart the recommended dosing, using one 200 mg tablet daily (4 mg/kg/day in pediatric patients) for the first 14 days (lead-in) followed by one 200 mg tablet twice daily (4 or 7 mg/kg twice daily, according to age, for pediatric patients).
An additional 200 mg dose of VIRAMUNE following each dialysis treatment is indicated in patients requiring dialysis. Nevirapine metabolites may accumulate in patients receiving dialysis; however, the clinical significance of this accumulation is not known (see CLINICAL PHARMACOLOGY , Pharmacokinetics in Special Populations : Renal Impairment ). Patients with CrCL >/=20 mL/min do not require an adjustment in VIRAMUNE dosing.
HOW SUPPLIED
VIRAMUNE (nevirapine) Tablets, 200 mg, are white, oval, biconvex tablets, 9.3 mm × 19.1 mm. One side is embossed with "54 193", with a single bisect separating the "54" and "193". The opposite side has a single bisect.
VIRAMUNE Tablets are supplied in bottles of 60 (NDC 0597-0046-60).
VIRAMUNE (nevirapine) Oral Suspension is a white to off-white preserved suspension containing 50 mg nevirapine (as nevirapine hemihydrate) in each 5 mL. VIRAMUNE suspension is supplied in plastic bottles with child-resistant closures containing 240 mL of suspension (NDC 0597-0047-24).
VIRAMUNE Tablets and VIRAMUNE Oral Suspension should be stored at 25°C (77°F); excursions permitted to 15°-30°C (59°F-86°F) [see USP Controlled Room Temperature]. Store in a safe place out of the reach of children.
Boehringer Ingelheim Pharmaceuticals, Inc.
Ridgefield, CT 06877 USA
© Copyright Boehringer Ingelheim Pharmaceuticals, Inc.
2005, ALL RIGHTS RESERVED
Revised: January 11, 2005
10003354/01 10003354/US/1
OT1801
MEDICATION GUIDE
VIRAMUNE ® (VIH-rah-mune) Tablets
VIRAMUNE ® Oral Suspension
Generic name: nevirapine tablets and oral suspension
Read this Medication Guide before you start taking VIRAMUNE® and each time you get a refill because there may be new information. This information does not take the place of talking with your doctor. You and your doctor should discuss VIRAMUNE when you start taking your medicine and at regular checkups. You should stay under a doctor's care while using VIRAMUNE. You should consult with your doctor before making any changes to your medications, except in any of the special circumstances described below regarding rash or liver problems.
What is the most important information I should know about VIRAMUNE ?
Patients taking VIRAMUNE may develop severe liver disease or skin reactions that can cause death. The risk of these reactions is greatest during the first 18 weeks of treatment, but these reactions also can occur later.
Liver Reactions
Any patient can experience liver problems while taking VIRAMUNE. However, women and patients who have higher CD4 counts when they begin VIRAMUNE treatment have a greater chance of developing liver damage. Women with CD4 counts higher than 250 cells/mm 3 are at the greatest risk of these events. If you are a woman with CD4>250 cells/mm 3 or a man with CD4>400 cells/mm 3 you should not begin taking VIRAMUNE unless you and your doctor have decided that the benefit of doing so outweighs the risk. Liver problems are often accompanied by a rash.
Patients starting VIRAMUNE with abnormal liver function tests and patients with hepatitis B or C have a greater chance of developing further increases in liver function tests after starting VIRAMUNE and throughout therapy.
In rare cases liver problems have led to liver failure and can lead to a liver transplant or death. Therefore, if you develop any of the following symptoms of liver problems stop taking VIRAMUNE and call your doctor right away:
- general ill feeling or "flu-like" symptoms
- tiredness
- nausea (feeling sick to your stomach)
- lack of appetite
- yellowing of your skin or whites of your eyes
- dark urine (tea colored)
- pale stools (bowel movements)
- pain, ache, or sensitivity to touch on your right side below your ribs
Your doctor should check you and do blood tests often to check your liver function during the first 18 weeks of therapy. Checks for liver problems should continue regularly during treatment with VIRAMUNE.
Skin Reactions
Skin rash is the most common side effect of VIRAMUNE. Most rashes occur in the first 6 weeks of treatment. In a small number of patients, rash can be serious and result in death . Therefore, if you develop a rash with any of the following symptoms stop using VIRAMUNE and call your doctor right away:
- general ill feeling or "flu-like" symptoms
- fever
- muscle or joint aches
- conjunctivitis (red or inflamed eyes, like "pink eye")
- any of the symptoms of liver problems discussed above
- blisters
- mouth sores
- swelling of your face
- tiredness
If your doctor tells you to stop treatment with VIRAMUNE because you have experienced the serious liver or skin reactions described above, never take VIRAMUNE again.
These are not all the side effects of VIRAMUNE. (See the section " What are the possible side effects of VIRAMUNE? " for more information.) Tell your doctor if you have any side effects from VIRAMUNE.
What is VIRAMUNE?
VIRAMUNE is a medicine used to treat Human Immunodeficiency Virus (HIV), the virus that causes AIDS (Acquired Immune Deficiency Syndrome).
VIRAMUNE is a type of anti-HIV medicine called a "non-nucleoside reverse transcriptase inhibitor" (NNRTI). It works by lowering the amount of HIV in the blood ("viral load"). You must take VIRAMUNE with other anti-HIV medicines. When taken with other anti-HIV medicines, VIRAMUNE can reduce viral load and increase the number of CD4 cells ("T cells"). CD4 cells are a type of immune helper cell in the blood. VIRAMUNE may not have these effects in every patient.
VIRAMUNE does not cure HIV or AIDS, and it is not known if it will help you live longer with HIV. People taking VIRAMUNE may still get infections common in people with HIV (opportunistic infections). Therefore, it is very important that you stay under the care of your doctor.
Who should not take VIRAMUNE?
- Do not take VIRAMUNE if you are allergic to VIRAMUNE or any of its ingredients. The active ingredient is nevirapine. Your doctor or pharmacist can tell you about the inactive ingredients.
- Do not restart VIRAMUNE after you recover from serious liver or skin reactions that happened when you took VIRAMUNE.
- Do not take VIRAMUNE if you take certain medicines. (See " Can I take other medicines with VIRAMUNE? " for a list of medicines.)
- Do not take VIRAMUNE if you are not infected with HIV.
What should I tell my doctor before taking VIRAMUNE?
Before starting VIRAMUNE, tell your doctor about all of your medical conditions, including if you:
- have problems with your liver or have had hepatitis
- are undergoing dialysis
- have skin conditions, such as a rash
- are pregnant, planning to become pregnant, or are breast feeding
How should I take VIRAMUNE?
- Take the exact amount of VIRAMUNE your doctor prescribes. The usual dose for adults is one tablet daily for the first 14 days followed by one tablet twice daily. Starting with one dose a day lowers the chance of rash, which could be serious. Therefore, it is important to strictly follow the once daily dose for the first 14 days. Do not start taking VIRAMUNE twice a day if you have any symptoms of liver problems or skin rash. (See the first section " What is the most important information I should know about VIRAMUNE? ")
- The dose of VIRAMUNE for children is based on their age and weight. Children's dosing also starts with once a day for 14 days and then twice a day after that.
- You may take VIRAMUNE with water, milk, or soda, with or without food.
- If you or your child uses VIRAMUNE suspension (liquid), shake it gently before use. Use an oral dosing syringe or dosing cup to measure the right dose. After drinking the medicine, fill the dosing cup with water and drink it to make sure you get all the medicine. If the dose is less than 5 mL (one teaspoon), use the syringe.
- Do not miss a dose of VIRAMUNE, because this could make the virus harder to treat. If you forget to take VIRAMUNE, take the missed dose right away. If it is almost time for your next dose, do not take the missed dose. Instead, follow your regular dosing schedule by taking the next dose at its regular time.
- If you stop taking VIRAMUNE for more than 7 days, ask your doctor how much to take before you start taking it again. You may need to start with once-a-day dosing.
- If you suspect that you have taken too much VIRAMUNE, contact your local poison control center or emergency room right away.
Can I take other medicines with VIRAMUNE?
- VIRAMUNE may change the effect of other medicines, and other medicines can change the effect of VIRAMUNE. Tell your doctors and pharmacists about all medicines you take, including non-prescription medicines, vitamins and herbal supplements.
- Do not take Nizoral® (ketoconazole) or Rifadin®/Rifamate®/Rifater® (rifampin) with VIRAMUNE.
- Tell your doctor if you take Biaxin® (clarithromycin), Diflucan® (fluconazole), methadone, or Mycobutin® (rifabutin). VIRAMUNE may not be right for you, or you may need careful monitoring.
- It is recommended that you not take products containing St. John's wort, which can reduce the amount of VIRAMUNE in your body.
- If you take birth control pills, you should not rely on them to prevent pregnancy. They may not work if you take VIRAMUNE. Talk with your doctor about other types of birth control that you can use.
What should I avoid while taking VIRAMUNE?
Avoid doing things that can spread HIV infection, as VIRAMUNE does not stop you from passing HIV infection to others. Do not share needles, other injection equipment or personal items that can have blood or body fluids on them, like toothbrushes and razor blades. Always practice safe sex by using a latex or polyurethane condom to lower the chance of sexual contact with semen, vaginal secretions, or blood.
The Centers for Disease Control and Prevention advises mothers with HIV not to breast feed so they will not pass HIV to the infant through their milk. Ask your doctor about the best way to feed your infant.
What are the possible side effects?
VIRAMUNE can cause serious liver damage and skin reactions that can cause death. Any patient can experience such side effects, but some patients are more at risk than others. (See " What is the most important information I should know about VIRAMUNE? " at the beginning of this Medication Guide.)
Other common side effects of VIRAMUNE include nausea, fatigue, fever, headache, vomiting, diarrhea, abdominal pain, and myalgia. This list of side effects is not complete. Ask your doctor or pharmacist for more information.
Changes in body fat have also been seen in some patients taking antiretroviral therapy. The changes may include increased amount of fat in the upper back and neck ("buffalo hump"), breast, and around the trunk. Loss of fat from the legs, arms, and face may also happen. The cause and long-term health effects of these conditions are not known at this time.
How do I store VIRAMUME?
Store VIRAMUNE at room temperature, between 59° to 86°F (15° to 30°C). Throw away VIRAMUNE that is no longer needed or out-of-date. Keep VIRAMUNE and all medicines out of the reach of children.
General information about VIRAMUNE
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use VIRAMUNE for a condition for which it was not prescribed. Do not give VIRAMUNE to other people, even if they have the same condition you have. It may harm them.
This Medication Guide summarizes the most important information about VIRAMUNE. If you would like more information, talk with your doctor. You can ask your pharmacist or doctor for information about VIRAMUNE that is written for health professionals, or you can visit www.viramune.com or call 1-800-542-6257 for additional information.
Boehringer Ingelheim Pharmaceuticals, Inc.
Ridgefield, CT 06877 USA
© Copyright Boehringer Ingelheim Pharmaceuticals, Inc.
2005, ALL RIGHTS RESERVED
Biaxin is a trademark of Abbott Laboratories. Diflucan is a trademark of Pfizer, Inc. Mycobutin is a trademark of Pharmacia & Upjohn Company. Nizoral is a trademark of Janssen Pharmaceutica. Rifadin, Rifamate and Rifater are trademarks of Aventis Pharmaceuticals Inc.
Revised: January 11, 2005
10003354/01 10003354/US/1
OT1801
This Medication Guide has been approved by the US Food and Drug Administration.
Subscribe to the "News" RSS Feed 
TOP ۞