-
Zemplar Capsules (Abbott)
DESCRIPTION
Paricalcitol, USP, the active ingredient in Zemplar Capsules, is a synthetically manufactured analog of calcitriol, the metabolically active form of vitamin D indicated for the prevention and treatment of secondary hyperparathyroidism in chronic kidney disease. Zemplar is available as soft gelatin capsules for oral administration containing 1 microgram, 2 micrograms or 4 micrograms of paricalcitol. Each capsule also contains medium chain triglycerides, alcohol, and butylated hydroxytoluene. The medium chain triglycerides are fractionated from coconut oil or palm kernel oil. The capsule shell is composed of gelatin, glycerin, titanium dioxide, iron oxide red (2 microgram capsules only), iron oxide yellow (2 microgram and 4 microgram capsules), iron oxide black (1 microgram capsules only), and water.
Paricalcitol is a white, crystalline powder with the empirical formula of C 27 H 44 O 3 , which corresponds to a molecular weight of 416.64. Paricalcitol is chemically designated as 19-nor-1(alpha),3(beta),25-trihydroxy-9, 10-secoergosta-5(Z),7(E),22(E)-triene and has the following structural formula:
CLINICAL PHARMACOLOGY
Secondary hyperparathyroidism is characterized by an elevation in parathyroid hormone (PTH) associated with inadequate levels of active vitamin D hormone. The source of vitamin D in the body is from synthesis in the skin and from dietary intake. Vitamin D requires two sequential hydroxylations in the liver and the kidney to bind to and to activate the vitamin D receptor (VDR). The endogenous VDR activator, calcitriol [1,25(OH) 2 D 3 ], is a hormone that binds to VDRs that are present in the parathyroid gland, intestine, kidney, and bone to maintain parathyroid function and calcium and phosphorus homeostasis, and to VDRs found in many other tissues, including prostate, endothelium and immune cells. VDR activation is essential for the proper formation and maintenance of normal bone. In the diseased kidney, the activation of vitamin D is diminished, resulting in a rise of PTH, subsequently leading to secondary hyperparathyroidism and disturbances in the calcium and phosphorus homeostasis. 1 Decreased levels of 1,25(OH) 2 D 3 have been observed in early stages of chronic kidney disease. The decreased levels of 1,25(OH) 2 D 3 and resultant elevated PTH levels, both of which often precede abnormalities in serum calcium and phosphorus, affect bone turnover rate and may result in renal osteodystrophy.
Mechanism of Action
Paricalcitol is a synthetic, biologically active vitamin D analog of calcitriol with modifications to the side chain (D 2 ) and the A (19-nor) ring. Preclinical and in vitro studies have demonstrated that paricalcitol's biological actions are mediated through binding of the VDR, which results in the selective activation of vitamin D responsive pathways. Vitamin D and paricalcitol have been shown to reduce parathyroid hormone levels by inhibiting PTH synthesis and secretion.
Pharmacokinetics
Absorption
Paricalcitol is well absorbed. In healthy subjects, following oral administration of paricalcitol at 0.24 mcg/kg, the mean absolute bioavailability was approximately 72%; the mean maximum plasma concentration (C max ), time to C max (T max ), and area under the concentration time curve (AUC 0-(infinity) ) were 0.630 ng/mL, 3 hours and 5.25 ng·h/mL, respectively. A food effect study in healthy subjects indicated that the C max and AUC 0-(infinity) were unchanged when paricalcitol was administered with a high fat meal compared to fasting. Food delays T max about 2 hours. The AUC 0-(infinity) of paricalcitol increased proportionally over the dose range of 0.06 to 0.48 mcg/kg in healthy subjects. Following multiple dosing, as once daily in CKD Stage 4 patients, the exposure (AUC) was slightly lower than that obtained after a single dose administration.
Distribution
Paricalcitol is extensively bound to plasma proteins (>/=99.8%). The mean apparent volume of distribution following a 0.24 mcg/kg dose of paricalcitol in healthy subjects was 34 L. The mean apparent volume of distribution following a 4 mcg dose of paricalcitol in CKD Stage 3 and 3 mcg dose in CKD Stage 4 patients is between 44 and 46 L.
Metabolism
After oral administration of a 0.48 mcg/kg dose of 3 H-paricalcitol, parent drug was extensively metabolized, with only about 2% of the dose eliminated unchanged in the feces, and no parent drug found in the urine. Several metabolites were detected in both the urine and feces. Most of the systemic exposure was from the parent drug. Two minor metabolites, relative to paricalcitol, were detected in human plasma. One metabolite was identified as 24(R)-hydroxy paricalcitol, while the other metabolite was unidentified. The 24(R)-hydroxy paricalcitol is less active than paricalcitol in an in vivo rat model of PTH suppression.
In vitro data suggest that paricalcitol is metabolized by multiple hepatic and non-hepatic enzymes, including mitochondrial CYP24, as well as CYP3A4 and UGT1A4. The identified metabolites include the product of 24(R)-hydroxylation, 24,26- and 24,28-dihydroxylation and direct glucuronidation.
Elimination
Paricalcitol is eliminated primarily via hepatobiliary excretion; approximately 70% of the radiolabeled dose is recovered in the feces and 18% is recovered in the urine. In healthy subjects, the mean elimination half-life of paricalcitol is 4 to 6 hours over the studied dose range of 0.06 to 0.48 mcg/kg. The pharmacokinetics of paricalcitol capsule have been studied in patients with chronic kidney disease (CKD) Stage 3 and 4 patients. After administration of 4 mcg paricalcitol capsule in CKD Stage 3 patients, the mean elimination half-life of paricalcitol is 17 hours. The mean half-life of paricalcitol is 20 hours in CKD Stage 4 patients when given 3 mcg of paricalcitol capsule.
Table 1. Paricalcitol Capsule Pharmacokinetic Characteristics in CKD Stage 3 and 4 PatientsPharmacokinetic
ParametersCKD Stage 3
n=15 *CKD Stage 4
n=14 *C max (ng/mL)0.11 ± 0.04 0.06 ± 0.01 AUC 0-(infinity) (ng·h/mL)2.42 ± 0.61 2.13 ± 0.73 CL/F (L/h)1.77 ± 0.50 1.52 ± 0.36 V/F (L)43.7 ± 14.4 46.4 ± 12.4 t 1/216.8 ± 2.65 19.7 ± 7.2 * Four mcg paricalcitol capsule was given to CKD Stage 3 patients; three mcg paricalcitol capsule was given to CKD Stage 4 patients.
Special Populations
Geriatric
The pharmacokinetics of paricalcitol have not been investigated in geriatric patients greater than 65 years (see PRECAUTIONS ).
Pediatric
The pharmacokinetics of paricalcitol have not been investigated in patients less than 18 years of age.
Gender
The pharmacokinetics of paricalcitol following single doses over 0.06 to 0.48 mcg/kg dose range were gender independent.
Hepatic Impairment
The disposition of paricalcitol (0.24 mcg/kg) was compared in patients with mild (n = 5) and moderate (n = 5) hepatic impairment (as indicated by the Child-Pugh method) and subjects with normal hepatic function (n = 10). The pharmacokinetics of unbound paricalcitol were similar across the range of hepatic function evaluated in this study. No dosing adjustment is required in patients with mild and moderate hepatic impairment. The influence of severe hepatic impairment on the pharmacokinetics of paricalcitol has not been evaluated.
Renal Impairment
Following administration of Zemplar Capsules, the pharmacokinetic profile of paricalcitol for CKD Stage 5 on hemodialysis (HD) or peritoneal dialysis (PD) was comparable to that in CKD 3 or 4 patients. Therefore, no special dosing adjustments are required other than those recommended in the Dosage and Administration section (see DOSAGE AND ADMINISTRATION ).
Drug Interactions
An in vitro study indicates that paricalcitol is not an inhibitor of CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1 or CYP3A at concentrations up to 50 nM (21 ng/mL) (approximately 20-fold greater than that obtained after highest tested dose). In fresh primary cultured hepatocytes, the induction observed at paricalcitol concentrations up to 50 nM was less than two-fold for CYP2B6, CYP2C9 or CYP3A, where the positive controls rendered a six- to nineteen-fold induction. Hence, paricalcitol is not expected to inhibit or induce the clearance of drugs metabolized by these enzymes.
Omeprazole: The pharmacokinetic interaction between paricalcitol capsule (16 mcg) and omeprazole (40 mg; oral) was investigated in a single dose, crossover study in healthy subjects. The pharmacokinetics of paricalcitol were unaffected when omeprazole was administered approximately 2 hours prior to the paricalcitol dose.
Ketoconazole: The effect of multiple doses of ketoconazole administered as 200 mg BID for 5 days on the pharmacokinetics of paricalcitol capsule has been studied in healthy subjects. The C max of paricalcitol was minimally affected, but AUC 0-(infinity) approximately doubled in the presence of ketoconazole. The mean half-life of paricalcitol was 17.0 hours in the presence of ketoconazole as compared to 9.8 hours, when paricalcitol was administered alone (see PRECAUTIONS ).
CLINICAL STUDIES
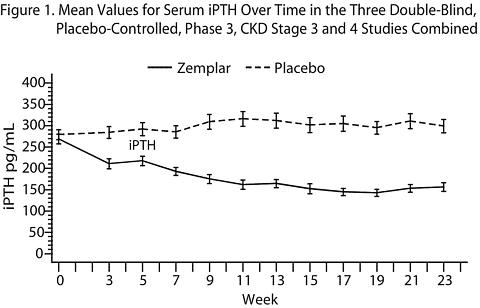
The safety and efficacy of Zemplar Capsules were evaluated in three, 24-week, double blind, placebo-controlled, randomized, multicenter, Phase 3 clinical studies in CKD Stage 3 and 4 patients. Two studies used an identical three times a week dosing design, and one study used a daily dosing design. A total of 107 patients received Zemplar Capsules and 113 patients received placebo. The mean age of the patients was 63 years, 68% were male, 71% were Caucasian, and 26% were African-American. The average baseline iPTH was 274 pg/mL (range: 145-856 pg/mL). The average duration of CKD prior to study entry was 5.7 years. At study entry 22% were receiving calcium based phosphate binders and/or calcium supplements. Baseline 25-hydroxyvitamin D levels were not measured.
The initial dose of Zemplar Capsules was based on baseline iPTH. If iPTH was </= 500 pg/mL, Zemplar Capsules were administered 1 mcg daily or 2 mcg three times a week, not more than every other day. If iPTH was > 500 pg/mL, Zemplar Capsules were administered 2 mcg daily or 4 mcg three times a week, not more than every other day. The dose was titrated by 1 mcg daily or 2 mcg three times a week every 2 to 4 weeks until iPTH levels were reduced by at least 30% from baseline. The overall average weekly dose of Zemplar Capsules was 9.6 mcg/week in the daily regimen and 9.5 mcg/week in the three times a week regimen.
In the clinical studies, doses were titrated for any of the following reasons: if iPTH fell to < 60 pg/mL, or decreased > 60% from baseline, the dose was reduced or temporarily withheld; if iPTH decreased < 30% from baseline and serum calcium was </= 10.3 mg/dL and serum phosphorus was </= 5.5 mg/dL, the dose was increased; and if iPTH decreased between 30 to 60% from baseline and serum calcium and phosphorus were </= 10.3 mg/dL and </= 5.5 mg/dL, respectively, the dose was maintained. Additionally, if serum calcium was between 10.4 to 11.0 mg/dL, the dose was reduced irrespective of iPTH, and the dose was withheld if serum calcium was > 11.0 mg/dL. If serum phosphorus was > 5.5 mg/dL, dietary counseling was provided, and phosphate binders could have been initiated or increased. If the elevation persisted, the Zemplar Capsules dose was decreased. Seventy-seven percent (77%) of the Zemplar Capsules treated patients and 82% of the placebo treated patients completed the 24-week treatment. The primary efficacy endpoint of at least two consecutive >/= 30% reductions from baseline iPTH was achieved by 91% of Zemplar Capsules treated patients and 13% of the placebo treated patients (p < 0.001). The proportion of Zemplar Capsules treated patients achieving two consecutive >/= 30% reductions was similar between the daily and the three times a week regimens (daily: 30/33, 91%; three times a week: 62/68, 91%).
The incidences of hypercalcemia (defined as two consecutive serum calcium values > 10.5 mg/dL), hyperphosphatemia and elevated Ca x P product in Zemplar Capsules treated patients was similar to placebo. There were no treatment related adverse events associated with hypercalcemia or hyperphosphatemia in the Zemplar Capsules group. No increases in urinary calcium or phosphorous were detected in Zemplar Capsules treated patients compared to placebo.
The pattern of change in the mean values for serum iPTH during the studies are shown in Figure 1.
The mean changes from baseline to final treatment visit in serum iPTH, calcium, phosphorus, calcium-phosphorus product (Ca × P), and bone- specific alkaline phosphatase are shown in Table 2.
Table 2. Mean Changes from Baseline to Final Treatment Visit in Serum iPTH, Bone Specific Alkaline Phosphatase, Calcium, Phosphorus, and Calcium x Phosphorus Product in Three Double-Blind, Placebo-Controlled, Phase 3, CKD Stage 3 and 4 Studies CombinedZemplar
CapsulesPlacebo iPTH (pg/mL)n = 104 n = 110 Mean Baseline Value266 279 Mean Final Treatment
Value162 315 Mean Change from Baseline
(SE)-104 (9.2) + 35 (9.0) Bone Specific Alkaline
Phosphatase (mcg/L)n = 101 n = 107 Mean Baseline17.1 18.8 Mean Final Treatment
Value9.2 17.4 Mean Change from Baseline
(SE)-7.9 (0.76) -1.4 (0.74) Calcium (mg/dL)n = 104 n = 110 Mean Baseline9.3 9.4 Mean Final Treatment
Value9.5 9.3 Mean Change from Baseline
(SE)+ 0.2 (0.04) -0.1 (0.04) Phosphorus (mg/dL)n = 104 n = 110 Mean Baseline4.0 4.0 Mean Final Treatment
Value4.3 4.3 Mean Change from Baseline
(SE)+ 0.3 (0.08) + 0.3 (0.08) Calcium × Phosphorus Product (mg 2 /dL 2 )n = 104 n = 110 Mean Baseline36.7 36.9 Mean Final Treatment
Value40.7 39.7 Mean Change from Baseline
(SE)+ 4.0 (0.74) + 2.9 (0.72)
INDICATIONS AND USAGE
Zemplar Capsules are indicated for the prevention and treatment of secondary hyperparathyroidism associated with chronic kidney disease (CKD) Stage 3 and 4.
CONTRAINDICATIONS
Zemplar Capsules should not be given to patients with evidence of vitamin D toxicity, hypercalcemia, or hypersensitivity to any ingredient in this product (see WARNINGS ).
WARNINGS
Excessive administration of vitamin D compounds, including Zemplar Capsules, can cause over suppression of PTH, hypercalcemia, hypercalciuria, hyperphosphatemia, and adynamic bone disease. Progressive hypercalcemia due to overdosage of vitamin D and its metabolites may be so severe as to require emergency attention. Acute hypercalcemia may exacerbate tendencies for cardiac arrhythmias and seizures and may potentiate the action of digitalis. Chronic hypercalcemia can lead to generalized vascular calcification and other soft-tissue calcification. High intake of calcium and phosphate concomitant with vitamin D compounds may lead to similar abnormalities and patient monitoring and individualized dose titration is required.
Pharmacologic doses of vitamin D and its derivatives should be withheld during Zemplar treatment to avoid hypercalcemia.
PRECAUTIONS
General
Digitalis toxicity is potentiated by hypercalcemia of any cause, so caution should be applied when digitalis compounds are prescribed concomitantly with Zemplar Capsules.
Information for Patients
The patient or guardian should be informed about compliance with dosage instructions, adherence to instructions about diet and phosphorus restriction, and avoidance of the use of unapproved nonprescription drugs. Phosphate-binding agents may be needed to control serum phosphorus levels in patients, but excessive use of aluminum containing compounds should be avoided. Patients also should be informed about the symptoms of elevated calcium (see ADVERSE REACTIONS ).
Laboratory Tests
During the initial dosing or following any dose adjustment of medication, serum calcium, serum phosphorus, and serum or plasma iPTH should be monitored at least every two weeks for 3 months after initiation of Zemplar therapy or following dose-adjustments in Zemplar therapy, then monthly for 3 months, and every 3 months thereafter.
Drug Interactions
Paricalcitol is not expected to inhibit the clearance of drugs metabolized by cytochrome P450 enzymes CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1 or CYP3A nor induce the clearance of drugs metabolized by CYP2B6, CYP2C9 or CYP3A.
A multiple dose drug-drug interaction study demonstrated that ketoconazole approximately doubled paricalcitol AUC 0-(infinity) (see CLINICAL PHARMACOLOGY ). Since paricalcitol is partially metabolized by CYP3A and ketoconazole is known to be a strong inhibitor of cytochrome P450 3A enzyme, care should be taken while dosing paricalcitol with ketoconazole and other strong P450 3A inhibitors including atazanavir, clarithromycin, indinavir, itraconazole, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin or voriconazole. Dose adjustment of Zemplar Capsules may be required, and iPTH and serum calcium concentrations should be closely monitored if a patient initiates or discontinues therapy with a strong CYP3A4 inhibitor such as ketoconazole.
Drugs that impair intestinal absorption of fat-soluble vitamins, such as cholestyramine, may interfere with the absorption of Zemplar Capsules.
Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 104-week carcinogenicity study in CD-1 mice, an increased incidence of uterine leiomyoma and leiomyosarcoma was observed at subcutaneous doses of 1, 3, 10 mcg/kg given three times weekly (2 to 15 times the AUC at a human dose of 14 mcg, equivalent to 0.24 mcg/kg based on AUC). The incidence rate of uterine leiomyoma was significantly different than the control group at the highest dose of 10 mcg/kg. In a 104-week carcinogenicity study in rats, there was an increased incidence of benign adrenal pheochromocytoma at subcutaneous doses of 0.15, 0.5, 1.5 mcg/kg (< 1 to 7 times the exposure following a human dose of 14 mcg, equivalent to 0.24 mcg/kg based on AUC). The increased incidence of pheochromocytomas in rats may be related to the alteration of calcium homeostasis by paricalcitol. Paricalcitol did not exhibit genetic toxicity in vitro with or without metabolic activation in the microbial mutagenesis assay (Ames Assay), mouse lymphoma mutagenesis assay (L5178Y), or a human lymphocyte cell chromosomal aberration assay. There was also no evidence of genetic toxicity in an in vivo mouse micronucleus assay. Paricalcitol had no effect on fertility (male or female) in rats at intravenous doses up to 20 mcg/kg/dose (equivalent to 13 times a human dose of 14 mcg based on surface area, mcg/m 2 ).
Pregnancy
Pregnancy category C
Paricalcitol has been shown to cause minimal decreases in fetal viability (5%) when administered daily to rabbits at a dose 0.5 times a human dose of 14 mcg or 0.24 mcg/kg (based on body surface area, mcg/m 2 ), and when administered to rats at a dose two times the 0.24 mcg/kg human dose (based on body surface area, mcg/m 2 ). At the highest dose tested, 20 mcg/kg administered three times per week in rats (13 times the 14 mcg human dose based on surface area, mcg/m 2 ), there was a significant increase in the mortality of newborn rats at doses that were maternally toxic and are known to produce hypercalcemia in rats. No other effects on offspring development were observed. Paricalcitol was not teratogenic at the doses tested.
Paricalcitol (20 mcg/kg) has been shown to cross the placental barrier in rats. There are no adequate and well-controlled clinical studies in pregnant women. Zemplar Capsules should be used during pregnancy only if the potential benefit to the mother justifies the potential risk to the fetus.
Nursing Mothers
Studies in rats have shown that paricalcitol is present in the milk. It is not known whether paricalcitol is excreted in human milk. In the nursing patient, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Geriatric Use
Of the total number (n = 220) of patients in clinical studies of Zemplar Capsules, 49% were 65 and over, while 17% were 75 and over. No overall differences in safety and effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
Pediatric Use
Safety and efficacy of Zemplar Capsules in pediatric patients have not been established.
ADVERSE REACTIONS
The safety of Zemplar Capsules has been evaluated in three 24-week (approximately six-month), double-blind, placebo-controlled, multicenter clinical studies involving 220 CKD Stage 3 and 4 patients. Six percent (6%) of Zemplar Capsules treated patients and 4% of placebo treated patients discontinued from clinical studies due to an adverse event. All reported adverse events occurring in at least 2% in either treatment group are presented in Table 3.
Table 3. Treatment - Emergent Adverse Events by Body System Occurring in >/= 2% of Subjects in the Zemplar-Treated Group of Three, Double-Blind, Placebo-Controlled, Phase 3, CKD Stage 3 and 4 Studies; All Treated PatientsNumber (%) of Subjects Body System a
COSTART V TermZemplar Capsules
(n = 107)Placebo
(n = 113)Overall88 (82%) 86 (76%) Body as a Whole49 (46%) 40 (35%) Accidental Injury10 (9%) 8 (7%) Pain8 (7%) 7 (6%) Viral Infection8 (7%) 8 (7%) Allergic Reaction6 (6%) 2 (2%) Headache5 (5%) 5 (4%) Abdominal Pain4 (4%) 2 (2%) Back Pain4 (4%) 1 (1%) Infection4 (4%) 4 (4%) Asthena3 (3%) 2 (2%) Chest Pain3 (3%) 1 (1%) Fever3 (3%) 1 (1%) Infection Fungal3 (3%) 0 (0%) Cyst2 (2%) 0 (0%) Flu Syndrome2 (2%) 1 (1%) Infection Bacterial2 (2%) 1 (1%) Cardiovascular27 (25%) 19 (17%) Hypertension7 (7%) 4 (4%) Hypotension5 (5%) 3 (3%) Syncope3 (3%) 1 (1%) Cardiomyopathy2 (2%) 0 (0%) Congestive Heart
Failure2 (2%) 5 (4%) Myocardial Infarct2 (2%) 0 (0%) Postural Hypotension2 (2%) 0 (0%) Digestive29 (27%) 31 (27%) Diarrhea7 (7%) 5 (4%) Nausea6 (6%) 4 (4%) Vomiting6 (6%) 5 (4%) Constipation4 (4%) 4 (4%) Gastroenteritis3 (3%) 3 (3%) Dyspepsia2 (2%) 2 (2%) Gastritis2 (2%) 4 (4%) Rectal Disorder2 (2%) 0 (0%) Hemic and Lymphatic
System4 (4%) 10 (9%) Hypervolemia2 (2%) 4 (4%) Ecchymosis2 (2%) 4 (4%) Metabolic and
Nutritional Disorders24 (22%) 34 (30%) Edema7 (7%) 5 (4%) Uremia7 (7%) 9 (8%) Gout4 (4%) 6 (5%) Dehydration3 (3%) 1 (1%) Acidosis2 (2%) 1 (1%) Hyperkalemia2 (2%) 3 (3%) Hyperphosphatemia2 (2%) 4 (4%) Hypoglycemia2 (2%) 4 (4%) Hypokalemia2 (2%) 1 (1%) Musculoskeletal12 (11%) 9 (8%) Arthritis5 (5%) 1 (1%) Leg Cramps3 (3%) 0 (0%) Myalgia2 (2%) 5 (4%) Nervous18 (17%) 12 (11%) Dizziness5 (5%) 5 (4%) Vertigo5 (5%) 0 (0%) Depression3 (3%) 0 (0%) Insomnia2 (2%) 2 (2%) Neuropathy2 (2%) 1 (1%) Respiratory26 (24%) 25 (22%) Pharyngitis11 (10%) 12 (11%) Rhinitis5 (5%) 4 (4%) Bronchitis3 (3%) 1 (1%) Cough Increased3 (3%) 2 (2%) Sinusitis3 (3%) 1 (1%) Epistaxis2 (2%) 1 (1%) Pneumonia2 (2%) 0 (0%) Skin and Appendages17 (16%) 10 (9%) Rash6 (6%) 3 (3%) Pruritus3 (3%) 3 (3%) Skin Ulcer3 (3%) 0 (0%) Skin Hypertrophy2 (2%) 0 (0%) Vesiculobullous Rash2 (2%) 1 (1%) Special Senses9 (8%) 11 (10%) Amblyopia2 (2%) 0 (0%) Retinal Disorder2 (2%) 0 (0%) Urogenital System10 (9%) 10 (9%) Urinary Tract
Infection3 (3%) 1 (1%) Kidney Function
Abnormal2 (2%) 1 (1%) a. Includes all patients with events in that body system.
Potential adverse effects of Zemplar Capsules are, in general, similar to those encountered with excessive vitamin D intake. The early and late signs and symptoms of hypercalcemia associated with vitamin D overdoses include:
Early: Weakness, headache, somnolence, nausea, vomiting, dry mouth, constipation, muscle pain, bone pain, and metallic taste.
Late: Anorexia, weight loss, conjunctivitis (calcific), pancreatitis, photophobia, rhinorrhea, pruritus, hyperthermia, decreased libido, elevated BUN, hypercholesterolemia, elevated AST and ALT, ectopic calcification, hypertension, cardiac arrhythmias, somnolence, death, and, rarely, overt psychosis.
OVERDOSAGE
Excessive administration of Zemplar Capsules can cause hypercalcemia, hypercalciuria, and hyperphosphatemia, and over suppression of PTH (see WARNINGS ).
Treatment of Overdosage
The treatment of acute overdosage of Zemplar Capsules should consist of general supportive measures. If drug ingestion is discovered within a relatively short time, induction of emesis or gastric lavage may be of benefit in preventing further absorption. If the drug has passed through the stomach, the administration of mineral oil may promote its fecal elimination. Serial serum electrolyte determinations (especially calcium), rate of urinary calcium excretion, and assessment of electrocardiographic abnormalities due to hypercalcemia should be obtained. Such monitoring is critical in patients receiving digitalis. Discontinuation of supplemental calcium and institution of a low-calcium diet are also indicated in accidental overdosage. Due to the relatively short duration of the pharmacological action of paricalcitol, further measures are probably unnecessary. If persistent and markedly elevated serum calcium levels occur, there are a variety of therapeutic alternatives that may be considered depending on the patient's underlying condition. These include the use of drugs such as phosphates and corticosteroids, as well as measures to induce an appropriate forced diuresis.
DOSAGE AND ADMINISTRATION
Zemplar Capsules may be administered daily or three times a week. When dosing three times weekly, the dose should be administered no more frequently than every other day. The average weekly doses for both daily and three times a week dosage regimens are similar (see CLINICAL STUDIES ).
Zemplar Capsules may be taken without regard to food. No dosing adjustment is required in patients with mild and moderate hepatic impairment.
Initial Dose
The initial dose of Zemplar Capsules is based on baseline intact parathyroid hormone (iPTH) levels.
Baseline iPTH
LevelDaily Dose Three Times a
Week Dose *</= 500 pg/mL 1 mcg 2 mcg > 500 pg/mL 2 mcg 4 mcg * To be administered not more often than every other day Dose Titration
Dosing must be individualized and based on serum or plasma iPTH levels, with monitoring of serum calcium and serum phosphorus. The following is a suggested approach in titration.
Dose Adjustment at
2 to 4 Week IntervalsiPTH Level
Relative to
BaselineZemplar
Capsule
DoseDaily
DosageThree
Times a
Week
Dosage *The same or
increasedIncrease 1 mcg 2 mcg Decreased by
< 30%Decreased by
>/= 30%, </= 60%Maintain Decreased > 60%Decrease 1 mcg 2 mcg iPTH < 60 pg/mL* To be administered not more often than every other day
If a patient is taking the lowest dose on the daily regimen and a dose reduction is needed, the dose can be decreased to 1 mcg three times a week. If a further dose reduction is required, the drug should be withheld as needed and can be restarted at a lower dose. If a patient is on a calcium-based phosphate binder, the binder dose may be decreased or withheld, or the patient may be switched to a non-calcium-based phosphate binder. If hypercalcemia or an elevated Ca × P is observed, the dose of Zemplar should be reduced or interrupted until these parameters are normalized.
Serum calcium and phosphorus levels should be closely monitored after initiation of Zemplar Capsules and during dose titration periods and coadministration with strong P450 3A inhibitors (see CLINICAL PHARMACOLOGY and PRECAUTIONS ).
HOW SUPPLIED
Zemplar Capsules are available as 1 mcg, 2 mcg, and 4 mcg capsules.
The 1 mcg capsule is an oval, gray, soft gelatin capsule imprinted with
and ZA, and is available in the following package size:
Bottles of 30 (NDC 0074-4317-30)
The 2 mcg capsule is an oval, orange-brown, soft gelatin capsule imprinted with
and ZF, and is available in the following package size:Bottles of 30 (NDC 0074-4314-30)
The 4 mcg capsule is an oval, gold soft gelatin capsule imprinted with
and ZK, and is available in the following package size:Bottles of 30 (NDC 0074-4315-30)
Storage
Store Zemplar Capsules at 25°C (77°F). Excursions permitted between 15°- 30°C (59°- 86°F). See USP Controlled Room Temperature.
U.S. patents: 5,246,925; 5,587,497
REFERENCES
1. K/DOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease. Am J Kidney Dis 2003; Volume 42(4): Supplement 3.
Ref: 03-5368-R1
Revised: May, 2005
05E-131-J605-3 MASTER
Abbott LABORATORIES 05E-131-J639-1North Chicago, IL 60064, U.S.A. Printed in USA
Subscribe to the "News" RSS Feed 
TOP ۞